Chapter 4 Immunopathology




























7 List key features of cytokines
 Cytokines are soluble signaling molecules secreted by a variety of cells, both of the immune and the nonimmune system.
Cytokines are soluble signaling molecules secreted by a variety of cells, both of the immune and the nonimmune system.







11 What are the characteristics of type I hypersensitivity (anaphylactic) reactions?
 Develop rapidly (within minutes) following exposure to the antigen in a previously sensitized individual
Develop rapidly (within minutes) following exposure to the antigen in a previously sensitized individual

12 Are the type I hypersensitivity reactions localized or systemic?
Type I hypersensitivity reaction may cause a localized or a systemic reaction.
 Localized reaction: If the allergen is confined to the site of contact, localized edema and inflammation typically develop (e.g., hives and rhinitis). This reaction causes only minor discomfort, but it may also be life threatening if it involves the larynx or the bronchial tree (e.g., bronchial asthma).
Localized reaction: If the allergen is confined to the site of contact, localized edema and inflammation typically develop (e.g., hives and rhinitis). This reaction causes only minor discomfort, but it may also be life threatening if it involves the larynx or the bronchial tree (e.g., bronchial asthma).
13 What is the pathogenesis of localized type I hypersensitivity reactions?
These reactions involve the interaction of three cell types:



First exposure leads to a sensitization and priming of the T and B cells, which interact and produce IgE that binds to the surface of mast cells in tissues. Upon second exposure to the same antigen, cross-linking of IgE on the mast cells occurs. Cell surface changes stimulate two sets of reactions (Fig. 4-1).


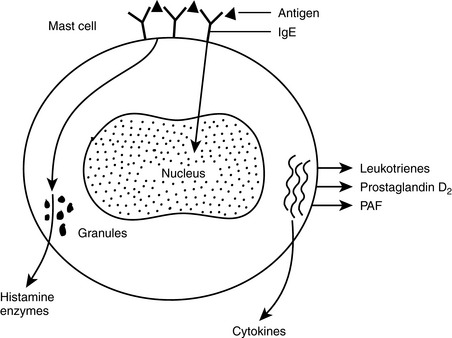
14 What occurs during the immediate degranulation of mast cells?
 Biogenic amines: Histamine, the primary mediator of this group, will increase vascular permeability (→ edema) and stimulate smooth muscle contraction (bronchospasm) and secretion of mucus or gastric juices.
Biogenic amines: Histamine, the primary mediator of this group, will increase vascular permeability (→ edema) and stimulate smooth muscle contraction (bronchospasm) and secretion of mucus or gastric juices.

15 Which mediators are released from mast cells in a delayed manner?
These mediators, known as secondary mediators and released 6 to 12 hours later, include:
 Lipid-derived mediators: Antigen binding to mast cells triggers an activation of phospholipase A2 that generates arachidonic acid from intracellular lipids. Arachidonic acid is further metabolized into leukotrienes and prostaglandins. Platelet-activating factor (PAF) is also formed.
Lipid-derived mediators: Antigen binding to mast cells triggers an activation of phospholipase A2 that generates arachidonic acid from intracellular lipids. Arachidonic acid is further metabolized into leukotrienes and prostaglandins. Platelet-activating factor (PAF) is also formed.
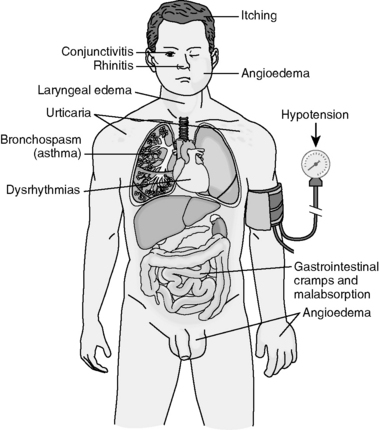
16 What are the symptoms associated with type I hypersensitivity reactions?
The symptoms depend on the route of exposure, dose of antigen, and the target organ sensitivity (Fig. 4-2).
 Systemic allergen presentation: Typically this reaction occurs upon injection of drugs, hormones, or antisera into a previously sensitized person. Clinically, an anaphylactic shock develops, which is characterized by hypotension due to widespread vascular dilatation, widespread edema, difficulty breathing due to laryngospasm, laryngeal and pulmonary edema, and cardiac dysrhythmia.
Systemic allergen presentation: Typically this reaction occurs upon injection of drugs, hormones, or antisera into a previously sensitized person. Clinically, an anaphylactic shock develops, which is characterized by hypotension due to widespread vascular dilatation, widespread edema, difficulty breathing due to laryngospasm, laryngeal and pulmonary edema, and cardiac dysrhythmia. Localized reactions: Antigen entering the body through the skin, by inhalation, or through ingestion evokes a reaction usually limited to one organ system.
Localized reactions: Antigen entering the body through the skin, by inhalation, or through ingestion evokes a reaction usually limited to one organ system. Upper respiratory tract reactions: Seasonal upper respiratory allergies caused by pollens (>10μm) evoke hay fever. Similar but prolonged allergic rhinitis may result from sensitization to dust mites. In both instances, there is nasal congestion, watery discharge, itching, sneezing, and cough.
Upper respiratory tract reactions: Seasonal upper respiratory allergies caused by pollens (>10μm) evoke hay fever. Similar but prolonged allergic rhinitis may result from sensitization to dust mites. In both instances, there is nasal congestion, watery discharge, itching, sneezing, and cough.


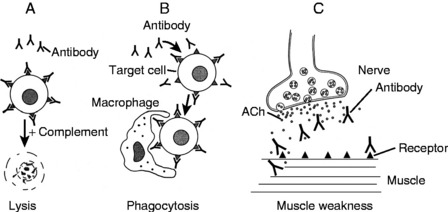
17 What are the characteristics of type II hypersensitivity (cytolytic) reactions?
Antigen is present on the surface of the target cell. It may be intrinsic antigen (e.g., Rh D blood antigen) or antigen adsorbed on the cell surface from the environment (e.g., drugs acting as haptens). The antibody interaction with the antigen elicits three reactions (Fig. 4-3):
 Complement-activated cell lysis: Binding of antibody (primarily IgM) to the antigen on the cell surface leads to an activation of complement-activated cell lysis and the formation of the cytolytic membrane attack complex (MAC), which destroys cells (e.g., acute hemolytic transfusion reaction).
Complement-activated cell lysis: Binding of antibody (primarily IgM) to the antigen on the cell surface leads to an activation of complement-activated cell lysis and the formation of the cytolytic membrane attack complex (MAC), which destroys cells (e.g., acute hemolytic transfusion reaction). Antibody-dependent cell-mediated cytotoxicity (ADCC): Binding of low-density (primarily IgG) antibodies that act as opsonins is followed by phagocytosis of damaged cells. ADCC typically mediates autoimmune hemolytic anemia and thrombocytopenia.
Antibody-dependent cell-mediated cytotoxicity (ADCC): Binding of low-density (primarily IgG) antibodies that act as opsonins is followed by phagocytosis of damaged cells. ADCC typically mediates autoimmune hemolytic anemia and thrombocytopenia.
18 List important diseases caused by type II hypersensitivity cytotoxic reactions
 Transfusion reaction: This is caused by a mismatched blood transfusion. An infusion of blood of an A blood group donor into a B blood group recipient will result in a massive hemolytic reaction mediated by the natural anti-A blood group antigen in the recipient.
Transfusion reaction: This is caused by a mismatched blood transfusion. An infusion of blood of an A blood group donor into a B blood group recipient will result in a massive hemolytic reaction mediated by the natural anti-A blood group antigen in the recipient.



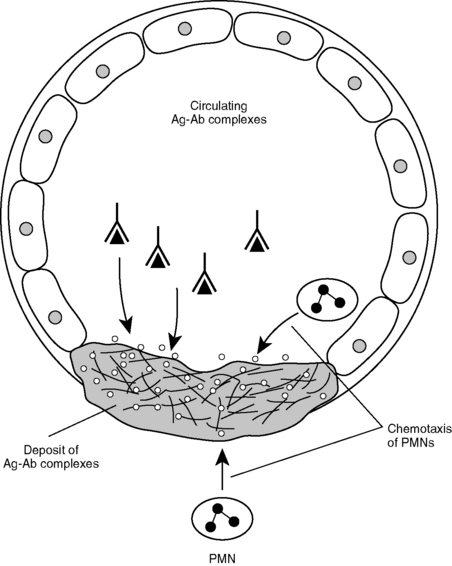
19 What are the characteristics of immune complex–mediated hypersensitivity (type III) reactions?
 Binding of antibody to the antigen forms complexes that are not cleared by the reticuloendothelial system but instead are deposited in tissues where they elicit an inflammatory reaction through activation of complement (Fig. 4-4).
Binding of antibody to the antigen forms complexes that are not cleared by the reticuloendothelial system but instead are deposited in tissues where they elicit an inflammatory reaction through activation of complement (Fig. 4-4).

20 List the most important diseases caused by type III hypersensitivity reaction
 Systemic lupus erythematosus (SLE): This disease is caused by circulating immune complexes that deposit in many organs, most often the skin, joints, and kidneys. Circulating blood cells are also often affected, resulting in anemia, leukopenia, and thrombocytopenia.
Systemic lupus erythematosus (SLE): This disease is caused by circulating immune complexes that deposit in many organs, most often the skin, joints, and kidneys. Circulating blood cells are also often affected, resulting in anemia, leukopenia, and thrombocytopenia.


< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


