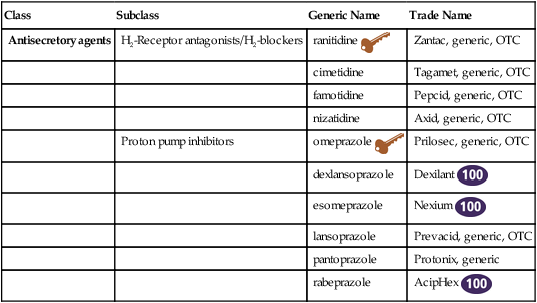
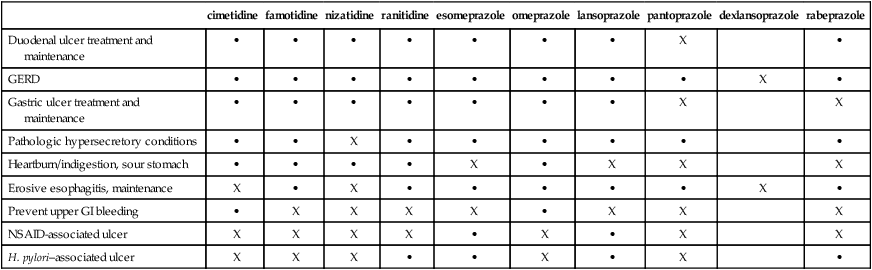
Chapter 27 H2-blockers (H2-receptor antagonists) and PPIs block acid secretion in the stomach but do so via different mechanisms of action. In general, all H2-blockers, except cimetidine, are considered equally effective and have similar side effect profiles. The indications and off-label uses for each agent are listed in Table 27-1. These distinctions are not always observed in practice. TABLE 27-1 Indications and Unlabeled Uses for H2-Blockers and PPIs
Histamine2-Blockers and Proton Pump Inhibitors
Class
Subclass
Generic Name
Trade Name
Antisecretory agents
H2-Receptor antagonists/H2-blockers
ranitidine 
Zantac, generic, OTC
cimetidine
Tagamet, generic, OTC
famotidine
Pepcid, generic, OTC
nizatidine
Axid, generic, OTC
Proton pump inhibitors
omeprazole 
Prilosec, generic, OTC
dexlansoprazole
Dexilant 
esomeprazole
Nexium 
lansoprazole
Prevacid, generic, OTC
pantoprazole
Protonix, generic
rabeprazole
AcipHex 
cimetidine
famotidine
nizatidine
ranitidine
esomeprazole
omeprazole
lansoprazole
pantoprazole
dexlansoprazole
rabeprazole
Duodenal ulcer treatment and maintenance
•
•
•
•
•
•
•
X
•
GERD
•
•
•
•
•
•
•
•
X
•
Gastric ulcer treatment and maintenance
•
•
•
•
•
•
•
X
X
Pathologic hypersecretory conditions
•
•
X
•
•
•
•
•
•
Heartburn/indigestion, sour stomach
•
•
•
•
X
•
X
X
X
Erosive esophagitis, maintenance
X
•
X
•
•
•
•
•
X
•
Prevent upper GI bleeding
•
X
X
X
X
•
X
X
X
NSAID-associated ulcer
X
X
X
X
•
X
•
X
X
H. pylori–associated ulcer
X
X
X
•
•
X
•
X
•
< div class='tao-gold-member'>
Histamine2-Blockers and Proton Pump Inhibitors

 Top 100 drug;
Top 100 drug;  key drug. Ranitidine is the most commonly used H2-receptor antagonist. Omeprazole is considered the key PPI because it is was the first to become available OTC and generic.
key drug. Ranitidine is the most commonly used H2-receptor antagonist. Omeprazole is considered the key PPI because it is was the first to become available OTC and generic.Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


