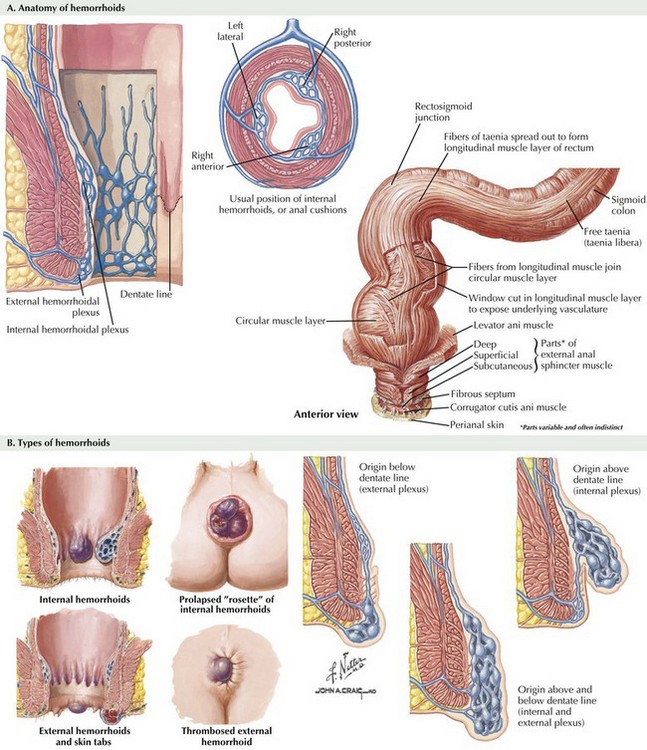
Chapter 26 Hemorrhoids are specialized, nonpathologic, vascular cushions found within the anal canal. They are typically organized into three anatomically distinct cushions located in the left lateral, right anterolateral, and right posterolateral anal canal (Fig. 26-1, A). Hemorrhoids are found in the submucosal layer and are considered sinusoids because they typically have no muscular wall. They are suspended in the anal canal by the muscle of Treitz, which is a submucosal extension of the conjoined longitudinal ligament. Hemorrhoids are classified as internal or external. Internal hemorrhoids are located proximal to the dentate line and have visceral innervation; therefore the most common presentation is painless bleeding. Because they are close to the anal transitional zone (ATZ), internal hemorrhoids can be covered by columnar, squamous, or basaloid cells. External hemorrhoids are located in the distal third of the anal canal and are covered by anoderm (squamous epithelium). Because of the somatic innervation of external hemorrhoids, patients who have these are more likely to be seen with pain (Fig. 26-1, B).
Hemorrhoids and Hemorrhoidectomy
Anatomy of Hemorrhoids
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


