 Hand Vessels
Hand VesselsVascular Anatomy of the Hand
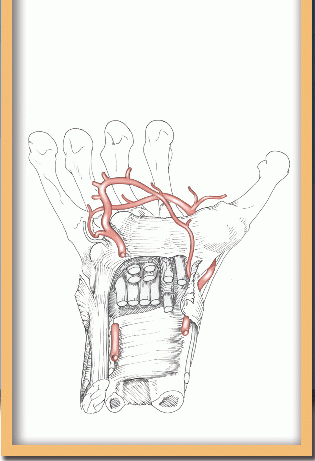
The anatomy of the hand is complex, and the ramification of the blood vessels within the tightly packed musculoskeletal structures is difficult to visualize. The following discussion presents hand anatomy as a framework for understanding the paths of the blood vessels.
Cutaneous Nerves of the Hand
The superficial innervation of the hand is relevant to the vascular surgeon in choosing an approach to the underlying vessels. Sensation is more critical to the function of the hand than to any other area of the body. All three major nerves of the arm provide sensation to areas of the hand, and the nerve branches in adjacent territories interconnect.
On the volar surface of the hand (Fig. 8-1), two major areas are supplied by the median and ulnar nerves. The division lies along the middle of the ring finger. A palmar cutaneous branch arises from the median nerve in the midforearm. This branch penetrates the deep fascia at the wrist and supplies the skin over the thenar eminence. The remainder of the palm and the volar surface of the fingers are innervated by the common and proper digital nerves branching from the main trunks of the median and ulnar nerves beneath the palmar fascia. The superficial palmaris brevis muscle at the base of the hypothenar eminence is innervated by the ulnar nerve. The radial side of the thenar eminence and dorsal thumb is served by the lateral branch of the superficial radial nerve.
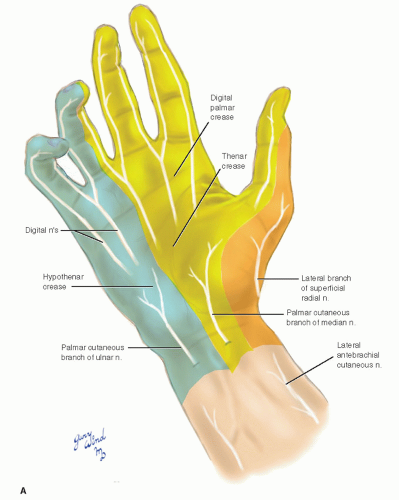 Fig. 8-1 The distribution of cutaneous nerves to the hand is shown. A: volar; B: dorsal. |
The dorsum of the hand is supplied by the ulnar and radial nerves. The dorsal branch of the ulnar
nerve arises in the distal forearm 5 cm from the wrist flexion crease and passes between the flexor carpi ulnaris and the distal ulna to reach the ulnar side of the dorsum of the hand. Its territory is again marked by the midline of the ring finger. The superficial branch of the radial nerve passes under the tendon of the brachioradialis muscle and crosses the anatomic snuffbox. It divides over the first extensor compartment into the lateral branch described previously and a larger medial division that supplies the remainder of the dorsum. A peculiarity of this distribution is that the distal phalanges of the index and middle fingers and the radial half of the ring finger are supplied by the median nerve. The superficial radial nerve is at risk of injury when surgically approaching the radial artery in the anatomic snuffbox.
nerve arises in the distal forearm 5 cm from the wrist flexion crease and passes between the flexor carpi ulnaris and the distal ulna to reach the ulnar side of the dorsum of the hand. Its territory is again marked by the midline of the ring finger. The superficial branch of the radial nerve passes under the tendon of the brachioradialis muscle and crosses the anatomic snuffbox. It divides over the first extensor compartment into the lateral branch described previously and a larger medial division that supplies the remainder of the dorsum. A peculiarity of this distribution is that the distal phalanges of the index and middle fingers and the radial half of the ring finger are supplied by the median nerve. The superficial radial nerve is at risk of injury when surgically approaching the radial artery in the anatomic snuffbox.
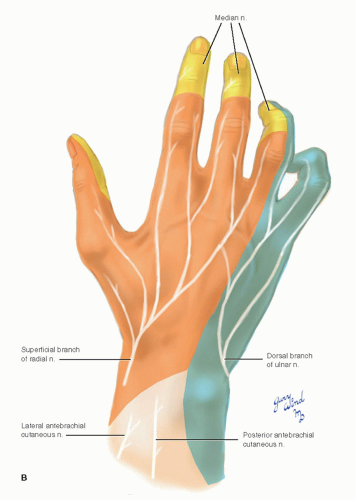 Fig. 8-1 (continued) |
Bones of the Hand
The key to understanding the bony framework of the hand is the carpal arch (Fig. 8-2). The deep volar concavity of the carpal bones forms the channel through which the major tendons pass from forearm to hand and establishes the foundation for opposition between the thumb and little finger. The tunnel for the flexor tendons is closed by a dense transverse ligament extending from the trapezium and scaphoid tubercle radially to the pisiform bone and hook of the hamate bone on the ulnar end of the arch. Note that the pisiform bone and hook of the hamate bone are not aligned axially relative to the ulna but angle toward the base of the third metacarpal.
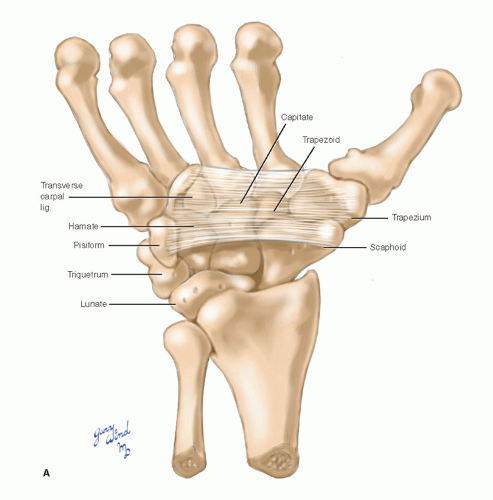 Fig. 8-2 The carpal bones form a deep arch that cradles the long flexor tendons. A: volar; B: proximal view. |
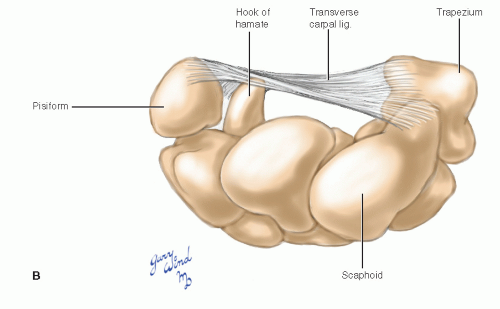 Fig. 8-2 (continued) |
Fascia
The deep fascia of the forearm is thickened around the wrist, forming the extensor retinaculum on the dorsum and the volar carpal ligament on the volar side (Fig. 8-3). The palmaris longus tendon fuses with the volar carpal ligament at the wrist and fans out over the central palm, reinforcing the deep fascia there and forming the palmar aponeurosis. This layer of investing fascia is distinct from the underlying transverse carpal ligament, which bridges the carpal arch from end to end and forms the restraining retinaculum for the flexor tendons. The transverse carpal ligament is derived from carpal ligaments with a contribution from the tendon of flexor carpi ulnaris muscle, whereas the volar carpal ligament is a thickened band of deep fascia. The only complexity in this relationship is the midline adherence between the palmar aponeurosis and the transverse carpal ligament. This adherence creates a canal on the ulnar side of the wrist, with the ulnar artery and nerve sandwiched between the two fascial layers (the canal of Guyon). The radial attachment of the transverse carpal ligament divides to accommodate the passage of the flexor carpi radialis tendon through a separate tunnel.
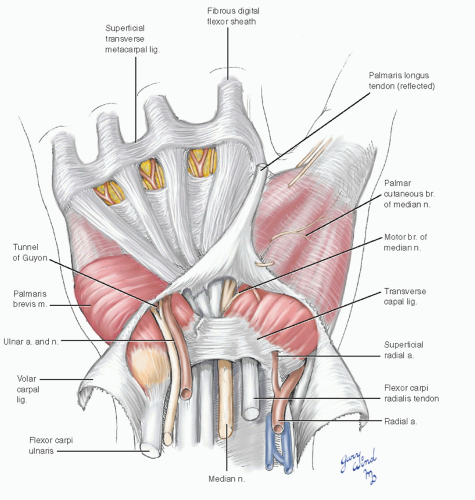 Fig. 8-3 The volar carpal ligament is a thickening of the deep fascia and is superficial to the transverse carpal ligament, which closes the carpal arch. |
Beyond the wrist, the palm is divided into three compartments by two fascial septa that span between the palmar aponeurosis and the first and fifth metacarpals, respectively (Fig. 8-4). These septa separate the thenar and hypothenar spaces from the central palmar compartment. The eight digital flexors are enclosed in a common bursa and fill the central compartment. The lumbrical muscles, digital nerves, and vessels also occupy this space.
A deep oblique connective tissue septum runs between the undersurface of the common bursa and the shaft of the middle metacarpal. This septum divides the plane between flexor tendons and the metacarpal/interossei layer into the midpalmar space on the ulnar side and the thenar space on the radial side. These potential spaces are the sites of deep hand infections.
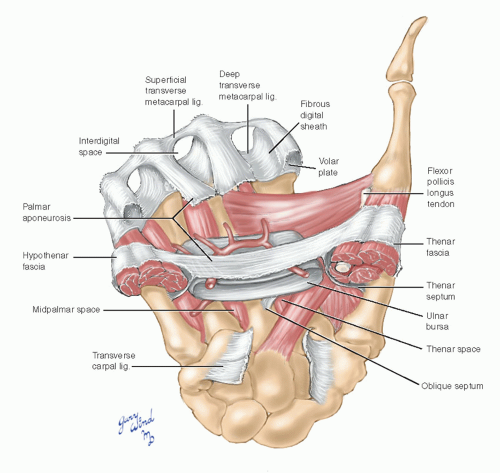 Fig. 8-4 The fascial compartments of the palm are shown. |
The palmar aponeurosis coalesces into four bands in the distal palm. These overlie and contribute to the fibrous flexor tendon sheaths at the distal end of the metacarpals. The interdigital space between the bands encloses the underlying digital nerves, arteries, and lumbrical muscles. Between the flexor sheaths, superficial and deep transverse metacarpal ligaments create three closed passages for these structures. The lumbrical muscles pass above the deep transverse metacarpal ligaments, and the tendons of the interosseous muscles pass below.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


