• Melanocytic markers may be useful to confirm presence of melanocytes
• Spitzoid features may be present in some cases (halo Spitz nevi)
• Reactive atypia may be seen
• Dermal component should show evidence of maturation with descent
• Mitoses should be rare to absent
Ancillary Tests
• Melanocytic markers may be useful to confirm presence of melanocytes
S100, SOX10, Melan-A, HMB-45, p16
Top Differential Diagnoses
• Melanoma
Can show associated inflammatory infiltrate but usually milder than halo nevi
Lack of symmetry and circumscription
Pagetoid scatter and dermal mitoses may be present
• Myerson nevus (eczematous nevus)
Clinical Photograph of Halo Nevi Two halo nevi seen on the back of a young adult are oval, well demarcated, and depigmented (skin colored or paler). With time, the white area may replace the nevus entirely .
Halo Nevus Showing Dense, Band-Like Inflammatory Infiltrate Halo nevus is characterized by a dense, band-like lymphohistiocytic infiltrate in the dermis . Several junctional and superficial nests of melanocytes can be appreciated upon close inspection.
Halo Nevus at Higher Magnification Higher magnification shows a dense lymphohistiocytic infiltrate with scattered melanophages . The melanocytes are mildly enlarged and atypical appearing but show no mitotic activity.
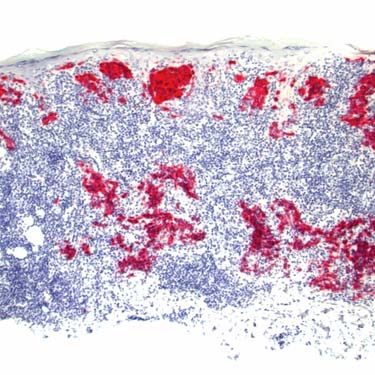
Melan-A Immunohistochemistry in Halo Nevus Melan-A immunohistochemistry in a halo nevus strongly highlights the residual junctional and dermal cells. S100 and Melan-A are usually diffusely positive, whereas HMB-45 usually only highlights the junctional cells (which can be useful in the differential with melanoma).
TERMINOLOGY
Synonyms
• Sutton nevus
• Nevus depigmentosa centrifugum
Definitions
• Nevus with clinically depigmented halo surrounding pigmented area
• Dense inflammatory infiltrate typically present
Histologically heavily inflamed nevi that lack clinical halo may be said to show halo reaction/phenomenon, but they are not true halo nevi
ETIOLOGY/PATHOGENESIS
Inflammatory Process
• Thought to be reaction to melanocytic antigens
• Infiltrate includes numerous T cells, including cytotoxic CD8(+) cells that may induce melanocyte apoptosis
CLINICAL ISSUES
Epidemiology
• Age
Usually young patients (children and young adults)
Patients over 40 years old uncommon
– Should raise concern for possibility of melanoma at another site
Site
• Most common on back but may occur at any site
Only gold members can continue reading. Log In or Register to continue





 .
.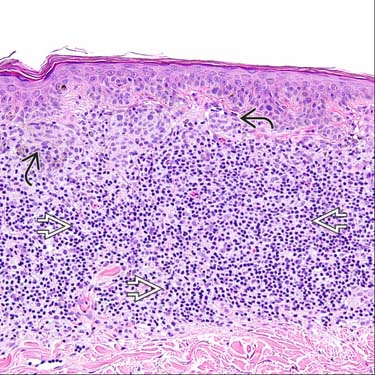
 . Several junctional and superficial nests of melanocytes
. Several junctional and superficial nests of melanocytes  can be appreciated upon close inspection.
can be appreciated upon close inspection.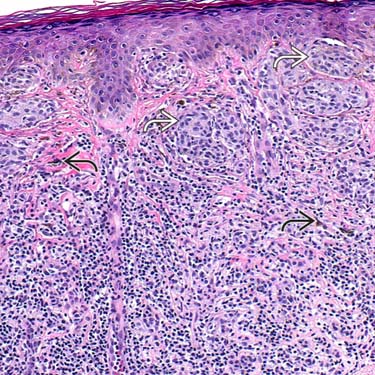
 . The melanocytes are mildly enlarged and atypical appearing
. The melanocytes are mildly enlarged and atypical appearing  but show no mitotic activity.
but show no mitotic activity.