114 | Bladder and Renal Cell Carcinomas |
BLADDER CANCER
Transitional cell epithelium lines the urinary tract from the renal pelvis to the ureter, urinary bladder, and the proximal two-thirds of the urethra. Cancers can occur at any point: 90% of malignancies develop in the bladder, 8% in the renal pelvis, and 2% in the ureter or urethra. Bladder cancer is the fourth most common cancer in men and the thirteenth in women, with an estimated 72,570 new cases and 15,210 deaths in the United States predicted for the year 2013. The almost 5:1 ratio of incidence to mortality reflects the higher frequency of the less lethal superficial variants compared to the more lethal invasive and metastatic variants. The incidence is roughly four times higher in men than in women and twofold higher in white men than in black men, with a median age of 65 years.
Once diagnosed, urothelial tumors exhibit polychronotropism, which is the tendency to recur over time in new locations in the urothelial tract. As long as urothelium is present, continuous monitoring is required.
EPIDEMIOLOGY
Cigarette smoking is believed to contribute to up to 50% of urothelial cancers in men and nearly 40% in women. The risk of developing a urothelial cancer in male smokers is increased two- to fourfold relative to nonsmokers and continues for 10 years or longer after cessation. Other implicated agents include aniline dyes, the drugs phenacetin and chlornaphazine, and external beam radiation. Chronic cyclophosphamide exposure also increases risk, whereas vitamin A supplements appear to be protective. Exposure to Schistosoma haematobium, a parasite found in many developing countries, is associated with an increase in both squamous and transitional cell carcinomas of the bladder.
PATHOLOGY
Clinical subtypes are grouped into three categories: 75% are superficial, 20% invade muscle, and 5% are metastatic at presentation. Staging of the tumor within the bladder is based on the pattern of growth and depth of invasion. The revised tumor, node, metastasis (TNM) staging system is illustrated in Fig. 114-1. About half of invasive tumors presented originally as superficial lesions that later progressed. Tumors are also rated by grade. Low-grade (highly differentiated) tumors rarely progress to a higher stage, whereas high-grade tumors do.
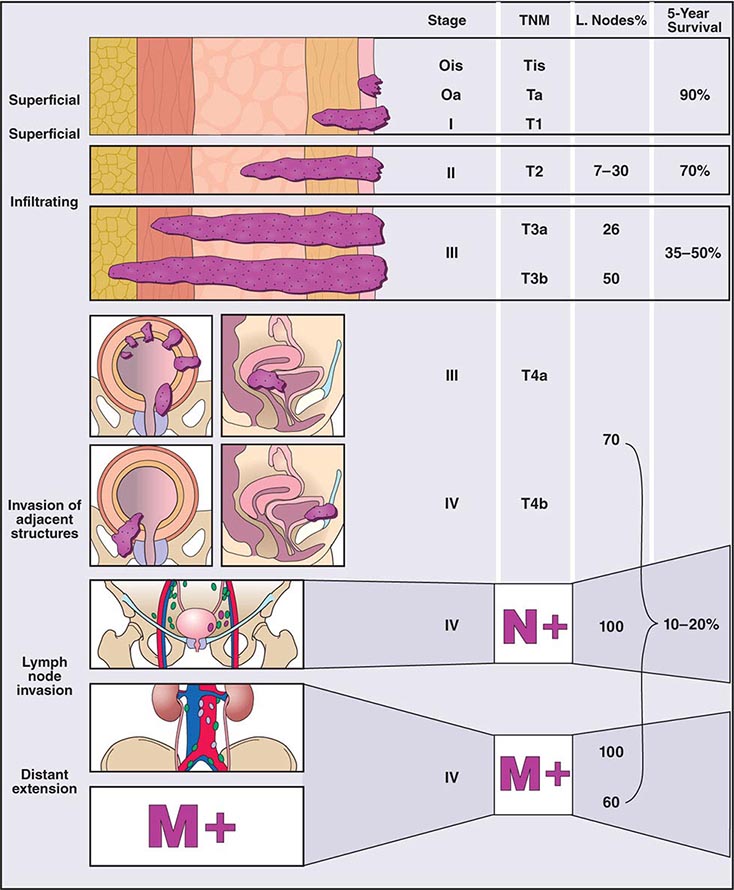
FIGURE 114-1 Bladder staging. TNM, tumor, node, metastasis.
More than 95% of urothelial tumors in the United States are transitional cell in origin. Pure squamous cancers with keratinization constitute 3%, adenocarcinomas 2%, and small cell tumors (often with paraneoplastic syndromes) <1%. Adenocarcinomas develop primarily in the urachal remnant in the dome of the bladder or in the periurethral tissues. Paragangliomas, lymphomas, and melanomas are rare. Of the transitional cell tumors, low-grade papillary lesions that grow on a central stalk are most common. These tumors are very friable, have a tendency to bleed, and have a high risk for recurrence, yet they rarely progress to the more lethal invasive variety. In contrast, carcinoma in situ (CIS) is a high-grade tumor that is considered a precursor of the more lethal muscle-invasive disease.
PATHOGENESIS
The multicentric nature of the disease and high recurrence suggests a field effect in the urothelium that results in a predisposition to develop cancer. Molecular genetic analyses suggest that the superficial and invasive lesions develop along distinct molecular pathways. Low-grade noninvasive papillary tumors harbor constitutive activation of the receptor tyrosine kinase-Ras signal transduction pathway and high frequencies of fibroblast growth factor receptor 3 and phosphoinositide-3 kinase α subunit mutations. In contrast, CIS and invasive tumors have a higher frequency of TP53 and RB gene alterations. Within all clinical stages, including Tis, T1, and T2 or greater lesions, tumors with alterations in p53, p21, and/or RB have a higher probability of recurrence, metastasis, and death from disease.
CLINICAL PRESENTATION, DIAGNOSIS, AND STAGING
Hematuria occurs in 80–90% of patients and often reflects exophytic tumors. The bladder is the most common source of gross hematuria (40%), but benign cystitis (22%) is a more common cause than bladder cancer (15%) (Chap. 61). Microscopic hematuria is more commonly of prostate origin (25%); only 2% of bladder cancers produce microscopic hematuria. Once hematuria is documented, a urinary cytology, visualization of the urothelial tract by computed tomography (CT) or magnetic resonance urogram or intravenous pyelogram, and cystoscopy are recommended if no other etiology is found. Screening asymptomatic individuals for hematuria increases the diagnosis of tumors at an early stage but has not been shown to prolong life. After hematuria, irritative symptoms are the next most common presentation. Ureteral obstruction may cause flank pain. Symptoms of metastatic disease are rarely the first presenting sign.
The endoscopic evaluation includes an examination under anesthesia to determine whether a palpable mass is present. A flexible endoscope is inserted into the bladder, and bladder barbotage for cytology is performed. Visual inspection includes mapping the location, size, and number of lesions, as well as a description of the growth pattern (solid vs papillary). All visible tumors should be resected, and a sample of the muscle underlying the tumor should be obtained to assess the depth of invasion. Normal-appearing areas are biopsied at random to ensure no CIS is present. A notation is made as to whether a tumor was completely or incompletely resected. Selective catheterization and visualization of the upper tracts should be performed if the cytology is positive and no disease is visible in the bladder. Ultrasonography, CT, and/or magnetic resonance imaging (MRI) are used to determine whether a tumor extends to perivesical fat (T3) and to document nodal spread. Distant metastases are assessed by CT of the chest and abdomen, MRI, or radionuclide imaging of the skeleton.
TREATMENT BLADDER CANCER
Management depends on whether the tumor invades muscle and whether it has spread to the regional lymph nodes and beyond. The probability of spread increases with increasing T stage.
NON–MUSCLE-INVASIVE DISEASE
At a minimum, the management is complete endoscopic resection with or without intravesical therapy. The decision to recommend intravesical therapy depends on the histologic subtype, number of lesions, depth of invasion, presence or absence of CIS, and antecedent history. Recurrences develop in upward of 50% of cases, of which 5–20% progress to a more advanced stage. In general, solitary papillary lesions are managed by transurethral surgery alone. CIS and recurrent disease are treated by transurethral surgery followed by intravesical therapy.
Intravesical therapies are used in two general contexts: as an adjuvant to a complete endoscopic resection to prevent recurrence or to eliminate disease that cannot be controlled by endoscopic resection alone. Intravesical treatments are advised for patients with diffuse CIS, recurrent disease, >40% involvement of the bladder surface by tumor, or T1 disease. The standard therapy, based on randomized comparisons, is Bacillus Calmette-Guérin (BCG) in six weekly instillations, often followed by maintenance administrations for ≥1 year. Other agents with activity include mitomycin C, interferon, and gemcitabine. The side effects of intravesical therapies include dysuria, urinary frequency, and, depending on the drug, myelosuppression or contact dermatitis. Rarely, intravesical BCG may produce a systemic illness associated with granulomatous infections in multiple sites requiring antituberculin therapy.
Following the endoscopic resection, patients are monitored for recurrence at 3-month intervals during the first year. Recurrence may develop anywhere along the urothelial tract, including the renal pelvis, ureter, or urethra. Persistent disease in the bladder and new tumors are treated with a second course of BCG or intravesical chemotherapy with valrubicin or gemcitabine. In some cases, cystectomy is recommended. Tumors in the ureter or renal pelvis are typically managed by resection during retrograde examination or, in some cases, by instillation through the renal pelvis. Prostatic urethral tumors may require cystoprostatectomy if the tumor cannot be resected completely.
MUSCLE-INVASIVE DISEASE
The treatment of a tumor that has invaded muscle can be separated into control of the primary tumor and systemic chemotherapy to treat micrometastatic disease. Radical cystectomy is the standard treatment in the United States, although in selected cases, a bladder-sparing approach is used. This approach includes complete endoscopic resection; partial cystectomy; or a combination of resection, systemic chemotherapy, and external beam radiation therapy. In some countries, external beam radiation therapy is considered standard. In the United States, it is generally limited to those patients deemed unfit for cystectomy, those with unresectable local disease, or as part of an experimental bladder-sparing approach.
Indications for cystectomy include muscle-invading tumors not suitable for segmental resection; non–muscle-invasive tumors unsuitable for conservative management (e.g., due to multicentric and frequent recurrences resistant to intravesical instillations); high-grade T1 tumors especially if associated with CIS; and bladder symptoms (e.g., frequency or hemorrhage) that impair quality of life.
Radical cystectomy is major surgery that requires appropriate preoperative evaluation and management. It involves removal of the bladder and pelvic lymph nodes and creation of a conduit or reservoir for urinary flow. Grossly abnormal lymph nodes are evaluated by frozen section. If metastases are confirmed, the procedure is often aborted. In males, radical cystectomy includes the removal of the prostate, seminal vesicles, and proximal urethra. Impotence is universal unless the nerves responsible for erectile function are preserved. In females, the procedure includes removal of the bladder, urethra, uterus, fallopian tubes, ovaries, anterior vaginal wall, and surrounding fascia.
Several options are frequently used for urinary diversion. Ileal conduits bring urine directly from the ureter to the abdominal wall. Some patients receive either a continent cutaneous reservoir constructed from detubularized bowel or an orthotopic neobladder. Approximately 25% of men receive a neobladder, leading to 85–90% continence during the day. Cutaneous reservoirs are drained by intermittent catheterization. Contraindications to a neobladder include renal insufficiency, an inability to self-catheterize, or CIS or an exophytic tumor in the urethra. Diffuse CIS in the bladder is a relative contraindication based on the risk of a urethral recurrence. Concurrent ulcerative colitis or Crohn’s disease may hinder the use of bowel.
A partial cystectomy may be considered when the disease is limited to the dome of the bladder, a ≥2 cm margin can be achieved, there is no associated CIS, and the bladder capacity is adequate after resection. This occurs in 5–10% of cases. Carcinomas in the ureter or in the renal pelvis are treated with nephroureterectomy with a bladder cuff to remove the tumor.
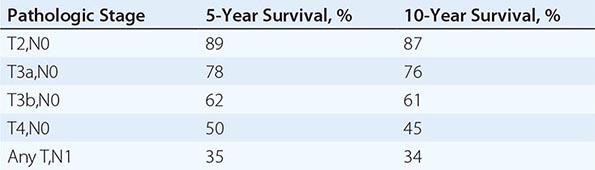
The probability of recurrence following surgery is based on pathologic stage, presence or absence of lymphatic or vascular invasion, and nodal spread. Among those whose cancers recur, the recurrence develops in a median of 1 year. Long-term outcomes vary by pathologic stage and histology (Table 114-1). The number of lymph nodes removed is also prognostic, whether or not the nodes contained tumor.
SURVIVAL FOLLOWING SURGERY FOR BLADDER CANCER |
Chemotherapy (described below) has been shown to prolong the survival of patients with muscle-invasive disease when combined with definitive treatment of the bladder by radical cystectomy or radiation therapy. Presurgical (or neoadjuvant) chemotherapy has been the most thoroughly explored, and increases the cure rate by 5–15%, whereas postsurgical (adjuvant) chemotherapy has not been proven definitively beneficial. For the majority of patients, chemotherapy alone is inadequate to eradicate the disease. Use of neoadjuvant chemotherapy is increasing, although it still remains underused. Experimental studies are evaluating bladder preservation strategies by combining chemotherapy and radiation therapy in patients whose tumors were endoscopically removed.
METASTATIC DISEASE
The primary goal of metastatic disease treatment is to achieve complete remission with chemotherapy alone or with a combined-modality approach of chemotherapy followed by surgical resection of residual disease. One can define a goal in terms of cure or palliation on the basis of the probability of achieving a complete response to chemotherapy using prognostic factors, such as Karnofsky performance status (KPS) (<80%) and whether the pattern of spread is nodal or visceral (liver, lung, or bone). For those with zero, one, or two risk factors, the probability of complete remission is 38, 25, and 5%, respectively, and median survival is 33, 13.4, and 9.3 months, respectively. Patients who have low KPS or who have visceral disease or bone metastases rarely achieve long-term survival. The toxicities also vary as a function of risk, and treatment-related mortality rates are as high as 3–4% using some combinations in these poor-risk patient groups. For most patients, treatment is palliative, aimed at delaying or relieving cancer-related symptoms, because few patients experience durable complete remissions.
CHEMOTHERAPY
A number of chemotherapeutic drugs have activity as single agents; cisplatin, paclitaxel, and gemcitabine are considered most active. Standard therapy consists of two-, three-, or four-drug combinations. Overall response rates of >50% have been reported using combinations such as methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC); gemcitabine and cisplatin (GC); or gemcitabine, paclitaxel, and cisplatin (GPC). MVAC was considered standard, but the toxicities of neutropenia and fever, mucositis, diminished renal and auditory function, and peripheral neuropathy led to the development of alternative regimens. At present, GC is used more commonly than MVAC based on the results of a comparative trial of MVAC versus GC that showed less neutropenia and fever and less mucositis for the GC regimen with similar response rates and median overall survival. Anemia and thrombocytopenia were more common with GC. GPC is not more effective than GC.
Chemotherapy has also been tested in the neoadjuvant and adjuvant settings. In a randomized trial, patients receiving three cycles of neoadjuvant MVAC followed by cystectomy had a significantly better median (6.2 years) and 5-year survival (57%) compared to cystectomy alone (median survival 3.8 years; 5-year survival 42%). Similar results were obtained in an international study of three cycles of cisplatin, methotrexate, and vinblastine (CMV) followed by either radical cystectomy or radiation therapy. The decision to administer adjuvant therapy is based on recurrence risk after cystectomy. Studies of adjuvant chemotherapy have been underpowered, and most closed for lack of accrual. One underpowered study using the GPC regimen suggested that adjuvant treatment improved survival, although many patients never received chemotherapy for metastases. Another underpowered study did not show a benefit for GC chemotherapy. Therefore, preoperative chemotherapy is preferred when medically appropriate. Indications for adjuvant chemotherapy in patients who did not receive neoadjuvant treatment include nodal disease, extravesical tumor extension, or vascular invasion in the resected specimen.
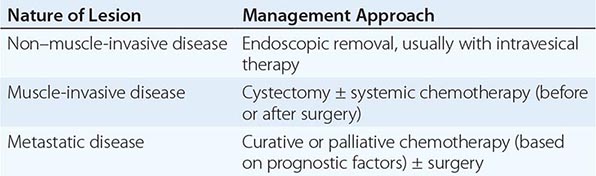
The management of bladder cancer is summarized in Table 114-2.
MANAGEMENT OF BLADDER CANCER |
CARCINOMA OF THE RENAL PELVIS AND URETER
About 5000 cases of renal pelvis and ureter cancer occur each year; nearly all are transitional cell carcinomas similar to bladder cancer in biology and appearance. This tumor is associated with chronic phenacetin abuse and aristolochic acid consumption in Chinese herbal preparations; aristolochic acid also seems to be associated with Balkan nephropathy, a chronic interstitial nephritis endemic in Bulgaria, Greece, Bosnia-Herzegovina, and Romania. In addition, upper tract urothelial carcinoma is linked to hereditary nonpolyposis colorectal cancer.
The most common symptom is painless gross hematuria, and the disease is usually detected on imaging during the workup for hematuria. Patterns of spread are like bladder cancer. For low-grade disease localized to the renal pelvis and ureter, nephroureterectomy (including excision of the distal ureter with a portion of the bladder) is associated with 5-year survival of 80–90%. More invasive or poorly differentiated tumors are more likely to recur locally and to metastasize. Metastatic disease is treated with the chemotherapy used in bladder cancer, and the outcome is similar to that of metastatic bladder cancer.
RENAL CELL CARCINOMA
Renal cell carcinomas account for 90–95% of malignant neoplasms arising from the kidney. Notable features include resistance to cytotoxic agents, infrequent responses to biologic response modifiers such as interleukin (IL) 2, robust activity to antiangiogenesis targeted agents, and a variable clinical course for patients with metastatic disease, including anecdotal reports of spontaneous regression.
EPIDEMIOLOGY
The incidence of renal cell carcinoma continues to rise and is now nearly 65,000 cases annually in the United States, resulting in 13,700 deaths. The male-to-female ratio is 2:1. Incidence peaks between the ages of 50 and 70 years, although this malignancy may be diagnosed at any age. Many environmental factors have been investigated as possible contributing causes; the strongest association is with cigarette smoking. Risk is also increased for patients who have acquired cystic disease of the kidney associated with end-stage renal disease and for those with tuberous sclerosis. Most cases are sporadic, although familial forms have been reported. One is associated with von Hippel-Lindau (VHL) syndrome. VHL syndrome is an autosomal dominant disorder. Genetic studies identified the VHL gene on the short arm of chromosome 3. Approximately 35% of individuals with VHL disease develop clear cell renal cell carcinoma. Other associated neoplasms include retinal hemangioma, hemangioblastoma of the spinal cord and cerebellum, pheochromocytoma, neuroendocrine tumors and cysts, and cysts in the epididymis of the testis in men and the broad ligament in women.
PATHOLOGY AND GENETICS
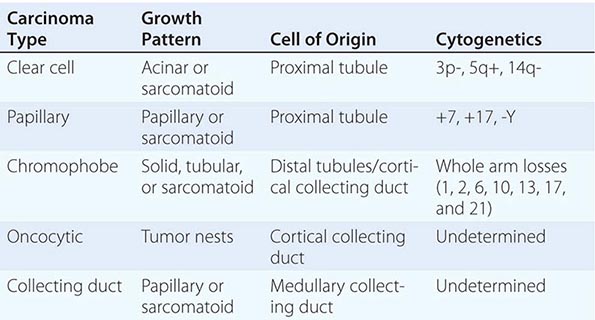
Renal cell neoplasia represents a heterogeneous group of tumors with distinct histopathologic, genetic, and clinical features ranging from benign to high-grade malignant (Table 114-3). They are classified on the basis of morphology and histology. Categories include clear cell carcinoma (60% of cases), papillary tumors (5–15%), chromophobe tumors (5–10%), oncocytomas (5–10%), and collecting or Bellini duct tumors (<1%). Papillary tumors tend to be bilateral and multifocal. Chromophobe tumors have a more indolent clinical course, and oncocytomas are considered benign neoplasms. In contrast, Bellini duct carcinomas, which are thought to arise from the collecting ducts within the renal medulla, are rare but often very aggressive. Clear cell tumors, the predominant histology, are found in >80% of patients who develop metastases. Clear cell tumors arise from the epithelial cells of the proximal tubules and usually show chromosome 3p deletions. Deletions of 3p21–26 (where the VHL gene maps) are identified in patients with familial as well as sporadic tumors. VHL encodes a tumor suppressor protein that is involved in regulating the transcription of vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and a number of other hypoxia-inducible proteins. Inactivation of VHL leads to overexpression of these agonists of the VEGF and PDGF receptors, which promote tumor angiogenesis and tumor growth. Agents that inhibit proangiogenic growth factor activity show antitumor effects. Enormous genetic variability has been documented in tumors from individual patients. Although the tumors have a clear clonal origin and often contain VHL mutations in common, different portions of the primary tumor and different metastatic sites may have wide variation in genetic lesions they contain. This tumor heterogeneity may underlie the emergence of treatment resistance.
CLASSIFICATION OF EPITHELIAL NEOPLASMS ARISING FROM THE KIDNEY |
CLINICAL PRESENTATION
The presenting signs and symptoms include hematuria, abdominal pain, and a flank or abdominal mass. Other symptoms are fever, weight loss, anemia, and a varicocele. The tumor is most commonly detected as an incidental finding on a radiograph. Widespread use of radiologic cross-sectional imaging procedures (CT, ultrasound, MRI) contributes to earlier detection, including incidental renal masses detected during evaluation for other medical conditions. The increasing number of incidentally discovered low-stage tumors has contributed to an improved 5-year survival for patients with renal cell carcinoma and increased use of nephron-sparing surgery (partial nephrectomy). A spectrum of paraneoplastic syndromes has been associated with these malignancies, including erythrocytosis, hypercalcemia, nonmetastatic hepatic dysfunction (Stauffer’s syndrome), and acquired dysfibrinogenemia. Erythrocytosis is noted at presentation in only about 3% of patients. Anemia, a sign of advanced disease, is more common.
The standard evaluation of patients with suspected renal cell tumors includes a CT scan of the abdomen and pelvis, chest radiograph, urine analysis, and urine cytology. If metastatic disease is suspected from the chest radiograph, a CT of the chest is warranted. MRI is useful in evaluating the inferior vena cava in cases of suspected tumor involvement or invasion by thrombus. In clinical practice, any solid renal masses should be considered malignant until proven otherwise; a definitive diagnosis is required. If no metastases are demonstrated, surgery is indicated, even if the renal vein is invaded. The differential diagnosis of a renal mass includes cysts, benign neoplasms (adenoma, angiomyolipoma, oncocytoma), inflammatory lesions (pyelonephritis or abscesses), and other primary or metastatic cancers. Other malignancies that may involve the kidney include transitional cell carcinoma of the renal pelvis, sarcoma, lymphoma, and Wilms’ tumor. All of these are less common causes of renal masses than is renal cell cancer.
STAGING AND PROGNOSIS
Staging is based on the American Joint Committee on Cancer (AJCC) staging system (Fig. 114-2). Stage I tumors are <7 cm in greatest diameter and confined to the kidney, stage II tumors are ≥7 cm and confined to the kidney, stage III tumors extend through the renal capsule but are confined to Gerota’s fascia (IIIa) or involve a single hilar lymph node (N1), and stage IV disease includes tumors that have invaded adjacent organs (excluding the adrenal gland) or involve multiple lymph nodes or distant metastases. The 5-year survival rate varies by stage: >90% for stage I, 85% for stage II, 60% for stage III, and 10% for stage IV.
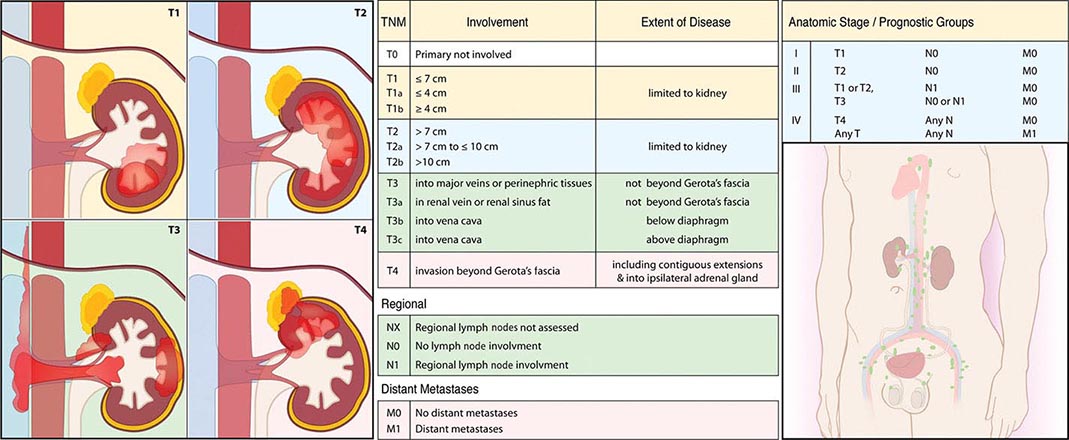
FIGURE 114-2 Renal cell carcinoma staging. TNM, tumor, node, metastasis.
115 | Benign and Malignant Diseases of the Prostate |
Benign and malignant changes in the prostate increase with age. Autopsies of men in the eighth decade of life show hyperplastic changes in >90% and malignant changes in >70% of individuals. The high prevalence of these diseases among the elderly, who often have competing causes of morbidity and mortality, mandates a risk-adapted approach to diagnosis and treatment. This can be achieved by considering these diseases as a series of states. Each state represents a distinct clinical milestone for which therapy(ies) may be recommended based on current symptoms, the risk of developing symptoms, or death from disease in relation to death from other causes within a given time frame. For benign proliferative disorders, symptoms of urinary frequency, infection, and potential for obstruction are weighed against the side effects and complications of medical or surgical intervention. For prostate malignancies, the risks of developing the disease, symptoms, or death from cancer are balanced against the morbidities of the recommended treatments and preexisting comorbidities.
ANATOMY
The prostate is located in the pelvis and is surrounded by the rectum, the bladder, the periprostatic and dorsal vein complexes and neurovascular bundles that are responsible for erectile function, and the urinary sphincter that is responsible for passive urinary control. The prostate is composed of branching tubuloalveolar glands arranged in lobules surrounded by fibromuscular stroma. The acinar unit includes an epithelial compartment made up of epithelial, basal, and neuroendocrine cells and separated by a basement membrane, and a stromal compartment that includes fibroblasts and smooth-muscle cells. Prostate-specific antigen (PSA) and prostatic acid phosphatase (PAP) are produced in the epithelial cells. Both prostate epithelial cells and stromal cells express androgen receptors (ARs) and depend on androgens for growth. Testosterone, the major circulating androgen, is converted by the enzyme 5α-reductase to dihydrotestosterone in the gland.
The periurethral portion of the gland increases in size during puberty and after the age of 55 years due to the growth of nonmalignant cells in the transition zone of the prostate that surrounds the urethra. Most cancers develop in the peripheral zone, and cancers in this location may be palpated during a digital rectal examination (DRE).
PROSTATE CANCER
In 2013, approximately 238,590 prostate cancer cases were diagnosed, and 29,720 men died from prostate cancer in the United States. The absolute number of prostate cancer deaths has decreased in the past 5 years, which has been attributed by some to the widespread use of PSA-based detection strategies. However, the benefit of screening on survival is unclear. The paradox of management is that although 1 in 6 men will eventually be diagnosed with the disease, and the disease remains the second leading cause of cancer deaths in men, only 1 man in 30 with prostate cancer will die of his disease.
EPIDEMIOLOGY
Epidemiologic studies show that the risk of being diagnosed with prostate cancer increases by a factor of two if one first-degree relative is affected and by four if two or more are affected. Current estimates are that 40% of early-onset and 5–10% of all prostate cancers are hereditary. Prostate cancer affects ethnic groups differently. Matched for age, African-American males have both a higher incidence of prostate cancer and larger tumors and more worrisome histologic features than white males. Polymorphic variants of the AR, the cytochrome P450 C17, and the steroid 5α-reductase type II (SRD5A2) genes have been implicated in the variations in incidence.
The prevalence of autopsy-detected cancers is similar around the world, while the incidence of clinical disease varies. Thus, environmental and dietary factors may play a role in prostate cancer growth and progression. High consumption of dietary fats, such as α-linoleic acid or the polycyclic aromatic hydrocarbons that form when red meats are cooked, is believed to increase risk. Similar to breast cancer in Asian women, the risk of prostate cancer in Asian men increases when they move to Western environments. Protective factors include consumption of the isoflavonoid genistein (which inhibits 5α-reductase) found in many legumes, cruciferous vegetables that contain the isothiocyanate sulforaphane, retinoids such as lycopene found in tomatoes, and inhibitors of cholesterol biosynthesis (e.g., statin drugs). The development of prostate cancer is a multistep process. One early change is hypermethylation of the GSTP1 gene promoter, which leads to loss of function of a gene that detoxifies carcinogens. The finding that many prostate cancers develop adjacent to a lesion termed proliferative inflammatory atrophy (PIA) suggests a role for inflammation.
PREVENTION
Currently no drugs or dietary supplements are approved by the U.S. Food and Drug Administration (FDA) for prevention of prostate cancer, nor are any recommended by the major clinical guidelines. Although statins may have some protective effect, the potential risks outweigh the benefits given the small number of men who die of prostate cancer. The results from several large, double-blind, randomized chemoprevention trials established 5α-reductase inhibitors (5ARI) as the most likely therapy to reduce the future risk of a prostate cancer diagnosis. The Prostate Cancer Prevention Trial (PCPT), in which men older than age 55 years received placebo or the 5ARI finasteride, which inhibits the type 1 isoform, showed a 25% (95% confidence interval 19–31%) reduction in the period prevalence of prostate cancer across all age groups in favor of finasteride (18.4%) over placebo (24.4%). In the Reduction by Dutasteride of Prostate Cancer Events (REDUCE) trial, a similar 23% reduction in the 4-year period prevalence was observed in favor of dutasteride (p = .001). Dutasteride inhibits both the type 1 and type 2 5ARI isoforms. While both studies met their endpoint, there was concern that most of the cancers that were prevented were low risk and that there was a slightly higher rate of clinically significant cancers (those with higher Gleason score) in the treatment arm. Neither drug was FDA-approved for prostate cancer prevention. In comparison, the Selenium and Vitamin E Cancer Prevention Trial (SELECT), which enrolled African-American men age ≥50 years and others age ≥55 years, showed no difference in cancer incidence in patients receiving vitamin E (4.6%) or selenium (4.9%) alone or in combination (4.6%) relative to placebo (4.4%). A similar lack of benefit for vitamin E, vitamin C, and selenium was seen in the Physicians Health Study II.
THE CLINICAL STATES MODEL
The prostate cancer continuum—from the appearance of a preneoplastic and invasive lesion localized to the prostate, to a metastatic lesion that results in symptoms and, ultimately, mortality—can span decades. To facilitate disease management, competing risks are considered in the context of a series of clinical states (Fig. 115-1). The states are defined operationally on the basis of whether or not a cancer diagnosis has been established and, for those with a diagnosis, whether or not metastases are detectable on imaging studies and the measured level of testosterone in the blood. With this approach, an individual resides in only one state and remains in that state until he has progressed. At each assessment, the decision to offer treatment and the specific form of treatment are based on the risk posed by the cancer relative to competing causes of mortality that may be present in that individual. It follows that the more advanced the disease, the greater is the need for treatment.
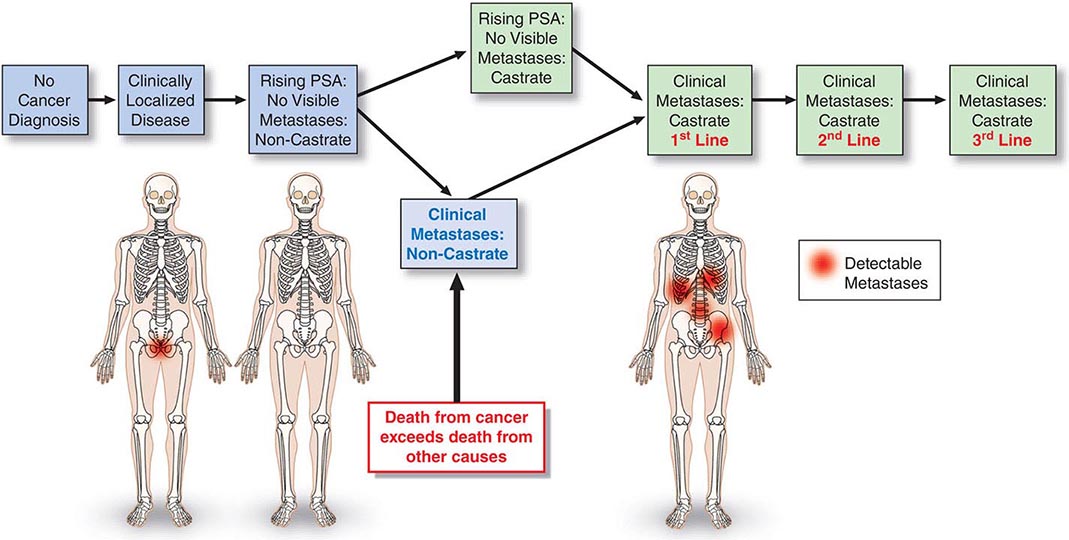
FIGURE 115-1 Clinical states of prostate cancer. PSA, prostate-specific antigen.
For those without a cancer diagnosis, the decision to undergo testing to detect a cancer is based on the individual’s estimated life expectancy and, separately, the probability that a clinically significant cancer may be present. For those with a prostate cancer diagnosis, the clinical states model considers the probability of developing symptoms or dying from prostate cancer. Thus, a patient with localized prostate cancer who has had all cancer removed surgically remains in the state of localized disease as long as the PSA remains undetectable. The time within a state becomes a measure of the efficacy of an intervention, although the effect may not be assessable for years. Because many men with active cancer are not at risk for metastases, symptoms, or death, the clinical states model allows a distinction between cure—the elimination of all cancer cells, the primary therapeutic objective when treating most cancers—and cancer control, in which the tempo of the illness is altered and symptoms are controlled until the patient dies of other causes. These can be equivalent therapeutically from a patient standpoint if the patient has not experienced symptoms of the disease or the treatment needed to control it. Even when a recurrence is documented, immediate therapy is not always necessary. Rather, as at the time of diagnosis, the need for intervention is based on the tempo of the illness as it unfolds in the individual, relative to the risk-to-benefit ratio of the therapy being considered.
SCREENING AND DIAGNOSIS
Physical Examination The need to pursue a diagnosis of prostate cancer is based on symptoms, an abnormal DRE, or, more typically, a change in or an elevated serum PSA. The urologic history should focus on symptoms of outlet obstruction, continence, potency, or change in ejaculatory pattern.
The DRE focuses on prostate size and consistency and abnormalities within or beyond the gland. Many cancers occur in the peripheral zone and may be palpated on DRE. Carcinomas are characteristically hard, nodular, and irregular, while induration may also be due to benign prostatic hypertrophy (BPH) or calculi. Overall, 20–25% of men with an abnormal DRE have cancer.
Prostate-Specific Antigen PSA (kallikrein-related peptidase 3; KLK3) is a kallikrein-related serine protease that causes liquefaction of seminal coagulum. It is produced by both nonmalignant and malignant epithelial cells and, as such, is prostate-specific, not prostate cancer–specific. Serum levels may also increase from prostatitis and BPH. Serum levels are not significantly affected by DRE, but the performance of a prostate biopsy can increase PSA levels up to tenfold for 8–10 weeks. PSA circulating in the blood is inactive and mainly occurs as a complex with the protease inhibitor α1-antichymotrypsin and as free (unbound) PSA forms. The formation of complexes between PSA, α2-macroglobulin, or other protease inhibitors is less significant. Free PSA is rapidly eliminated from the blood by glomerular filtration with an estimated half-life of 12–18 h. Elimination of PSA bound to α1-antichymotrypsin is slow (estimated half-life of 1–2 weeks) because it too is largely cleared by the kidneys. Levels should be undetectable after about 6 weeks if the prostate has been removed. Immunohistochemical staining for PSA can be used to establish a prostate cancer diagnosis.
PSA-BASED SCREENING AND EARLY DETECTION PSA testing was approved by the U.S. FDA in 1994 for early detection of prostate cancer, and the widespread use of the test has played a significant role in the proportion of men diagnosed with early-stage cancers: more than 70–80% of newly diagnosed cancers are clinically organ-confined. The level of PSA in blood is strongly associated with the risk and outcome of prostate cancer. A single PSA measured at age 60 is associated (area under the curve [AUC] of 0.90) with lifetime risk of death from prostate cancer. Most prostate cancer deaths (90%) occur among men with PSA levels in the top quartile (>2 ng/mL), although only a minority of men with PSA >2 ng/mL will develop lethal prostate cancer. Despite this and mortality rate reductions reported from large randomized prostate cancer screening trials, routine use of the test remains controversial.
The U.S. Preventive Services Task Force (USPSTF) reviewed the evidence for screening for prostate cancer and made a clear recommendation against screening. By giving a grade of “D” in the recommendation statement that was based on this review, the USPSTF concluded that “there is moderate or high certainty that this service has no net benefit or that the harms outweigh the benefits.” Whether the harms of screening, overdiagnosis, and overtreatment are justified by the benefits in terms of reduced prostate cancer mortality is open to reasonable doubt. In response to the USPSTF, the American Urological Association (AUA) updated their consensus statement regarding prostate cancer screening. They concluded that the quality of evidence for the benefits of screening was moderate, and evidence for harm was high for men age 55–69 years. For men outside this age range, evidence was lacking for benefit, but the harms of screening, including overdiagnosis and overtreatment, remained. The AUA recommends shared decision making considering PSA-based screening for men age 55–69, a target age group for whom benefits may outweigh harms. Outside this age range, PSA-based screening as a routine test was not recommended based on the available evidence. The entire guideline is available at www.AUAnet.org/education/guidelines/prostate-cancer-detection.cfm.
The PSA criteria used to recommend a diagnostic prostate biopsy have evolved over time. However, based on the commonly used cut point for prostate biopsy (a total PSA ≥4 ng/mL), most men with a PSA elevation do not have histologic evidence of prostate cancer at biopsy. In addition, many men with PSA levels below this cut point harbor cancer cells in their prostate. Information from the PCPT demonstrates that there is no PSA below which the risk of prostate cancer is zero. Thus, the PSA level establishes the likelihood that a man will harbor cancer if he undergoes a prostate biopsy. The goal is to increase the sensitivity of the test for younger men more likely to die of the disease and to reduce the frequency of detecting cancers of low malignant potential in elderly men more likely to die of other causes. Patients with symptomatic prostatitis should have a course of antibiotics before biopsy. However, the routine use of antibiotics in an asymptomatic man with an elevated PSA level is strongly discouraged.
Prostate Biopsy A diagnosis of cancer is established by an image-guided needle biopsy. Direct visualization by transrectal ultrasound (TRUS) or magnetic resonance imaging (MRI) assures that all areas of the gland are sampled. Contemporary schemas advise an extended-pattern 12-core biopsy that includes sampling from the peripheral zone as well as a lesion-directed palpable nodule or suspicious image-guided sampling. Men with an abnormal PSA and negative biopsy are advised to undergo a repeat biopsy.
BIOPSY PATHOLOGY Each core of the biopsy is examined for the presence of cancer, and the amount of cancer is quantified based on the length of the cancer within the core and the percentage of the core involved. Of the cancers identified, >95% are adenocarcinomas; the rest are squamous or transitional cell tumors or, rarely, carcinosarcomas. Metastases to the prostate are rare, but in some cases colon cancers or transitional cell tumors of the bladder invade the gland by direct extension.
When prostate cancer is diagnosed, a measure of histologic aggressiveness is assigned using the Gleason grading system, in which the dominant and secondary glandular histologic patterns are scored from 1 (well-differentiated) to 5 (undifferentiated) and summed to give a total score of 2–10 for each tumor. The most poorly differentiated area of tumor (i.e., the area with the highest histologic grade) often determines biologic behavior. The presence or absence of perineural invasion and extracapsular spread is also recorded.
Prostate Cancer Staging The tumor, node, metastasis (TNM) staging system includes categories for cancers identified solely on the basis of an abnormal PSA (T1c), those that are palpable but clinically confined to the gland (T2), and those that have extended outside the gland (T3 and T4) (Table 115-1, Fig. 115-2). DRE alone is inaccurate in determining the extent of disease within the gland, the presence or absence of capsular invasion, involvement of seminal vesicles, and extension of disease to lymph nodes. Because of the inadequacy of DRE for staging, the TNM staging system was modified to include the results of imaging. Unfortunately, no single test has proven to accurately indicate the stage or the presence of organ-confined disease, seminal vesicle involvement, or lymph node spread.
TNM CLASSIFICATION |
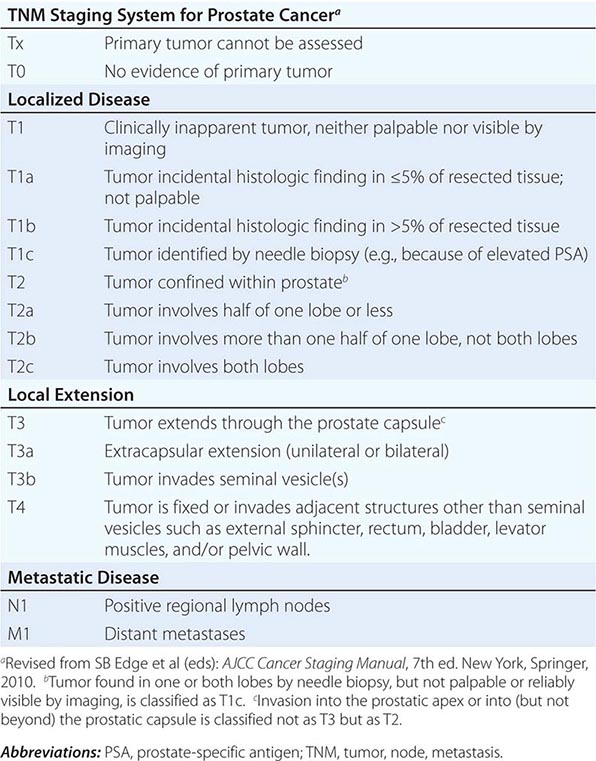
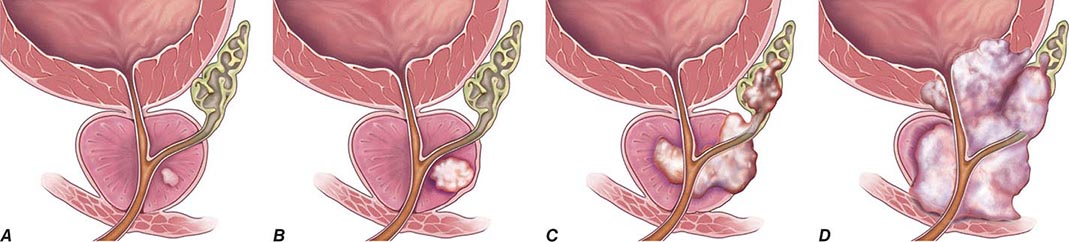
FIGURE 115-2 T stages of prostate cancer. (A) T1—Clinically inapparent tumor, neither palpable nor visible by imaging; (B) T2—Tumor confined within prostate; (C) T3—Tumor extends through prostate capsule and may invade the seminal vesicles; (D) T4—Tumor is fixed or invades adjacent structures. Eighty-one percent of patients present with local disease (T1 and T2), which is associated with a 5-year survival rate of 100%. An additional 12% of patients present with regional disease (T3 and T4 without metastases), which is also associated with a 100% survival rate after 5 years. Four percent of patients present with distant disease (T4 with metastases), which is associated with a 28% 5-year survival rate. (Three percent of patients are ungraded, and this group is associated with a 73% 5-year survival rate.) (Data from AJCC, http://seer.cancer.gov/statfacts/html/prost.html. Figure © 2014 Memorial Sloan-Kettering Cancer Center; used with permission.)
TRUS is the imaging technique most frequently used to assess the primary tumor, but its chief use is directing prostate biopsies, not staging. No TRUS finding consistently indicates cancer with certainty. Computed tomography (CT) lacks sensitivity and specificity to detect extraprostatic extension and is inferior to MRI in visualization of lymph nodes. In general, MRI performed with an endorectal coil is superior to CT to detect cancer in the prostate and to assess local disease extent. T1-weighted MRI produces a high signal in the periprostatic fat, periprostatic venous plexus, perivesicular tissues, lymph nodes, and bone marrow. T2-weighted MRI demonstrates the internal architecture of the prostate and seminal vesicles. Most cancers have a low signal, while the normal peripheral zone has a high signal, although the technique lacks sensitivity and specificity. MRI is also useful for the planning of surgery and radiation therapy.
Radionuclide bone scans (bone scintigraphy) are used to evaluate spread to osseous sites. This test is sensitive but relatively nonspecific because areas of increased uptake are not always related to metastatic disease. Healing fractures, arthritis, Paget’s disease, and other conditions will also cause abnormal uptake. True-positive bone scans are uncommon when the PSA is <10 ng/mL unless the tumor is high grade.
TREATMENT | TREATMENT OF PROSTATE CANCER BY CLINICAL STATE |
CLINICALLY LOCALIZED PROSTATE CANCER
Clinically localized prostate cancers are those that appear to be nonmetastatic after staging studies are performed. Patients with clinically localized disease are managed by radical prostatectomy, radiation therapy, or active surveillance. Choice of therapy requires the consideration of several factors: the presence of symptoms, the probability that the untreated tumor will adversely affect the quality or duration of survival and thus require treatment, and the probability that the tumor can be cured by single-modality therapy directed at the prostate or that it will require both local and systemic therapy to achieve cure.
Data from the literature do not provide clear evidence for the superiority of any one treatment relative to another. Comparison of outcomes of various forms of therapy is limited by the lack of prospective trials, referral bias, the experience of the treating teams, and differences in endpoints and cancer control definitions. Often, PSA relapse–free survival is used because an effect on metastatic progression or survival may not be apparent for years. After radical surgery to remove all prostate tissue, PSA should become undetectable in the blood within 6 weeks. If PSA remains or becomes detectable after radical prostatectomy, the patient is considered to have persistent disease. After radiation therapy, in contrast, PSA does not become undetectable because the remaining nonmalignant elements of the gland continue to produce PSA even if all cancer cells have been eliminated. Similarly, cancer control is not well defined for a patient managed by active surveillance because PSA levels will continue to rise in the absence of therapy. Other outcomes are time to objective progression (local or systemic), cancer-specific survival, and overall survival; however, these outcomes may take years to assess.
The more advanced the disease, the lower the probability of local control and the higher the probability of systemic relapse. More important is that within the categories of T1, T2, and T3 disease are cancers with a range of prognoses. Some T3 tumors are curable with therapy directed solely at the prostate, and some T1 lesions have a high probability of systemic relapse that requires the integration of local and systemic therapy to achieve cure. For T1c cancers in particular, stage alone is inadequate to predict outcome and select treatment; other factors must be considered.
Nomograms To better assess risk and guide treatment selection, many groups have developed prognostic models or nomograms that use a combination of the initial clinical T stage, biopsy Gleason score, and baseline PSA. Some use discrete cut points (PSA <10 or ≥10 ng/mL; Gleason score of ≤6, 7, or ≥8); others employ nomograms that use PSA and Gleason score as continuous variables. More than 100 nomograms have been reported to predict the probability that a clinically significant prostate cancer is present, disease extent (organ-confined vs non–organ-confined, node-negative or -positive), or the probability of success of treatment for specific local therapies using pretreatment variables. Considerable controversy exists over what constitutes “high risk” based on a predicted probability of success or failure. In these situations, nomograms and predictive models can only go so far. Exactly what probability of success or failure would lead a physician to recommend and a patient to seek alternative approaches is controversial. As an example, it may be appropriate to recommend radical surgery for a younger patient with a low probability of cure. Nomograms are being refined continually to incorporate additional clinical parameters, biologic determinants, and year of treatment, which can also affect outcomes, making treatment decisions a dynamic process.
Treatment-Related Adverse Events The frequency of adverse events varies by treatment modality and the experience of the treating team. For example, following radical prostatectomy, incontinence rates range from 2–47% and impotence rates range from 25–89%. Part of the variability relates to how the complication is defined and whether the patient or physician is reporting the event. The time of the assessment is also important. After surgery, impotence is immediate but may reverse over time, while with radiation therapy impotence is not immediate but may develop over time. Of greatest concern to patients are the effects on continence, sexual potency, and bowel function.
Radical Prostatectomy The goal of radical prostatectomy is to excise the cancer completely with a clear margin, to maintain continence by preserving the external sphincter, and to preserve potency by sparing the autonomic nerves in the neurovascular bundle. The procedure is advised for patients with a life expectancy of 10 years or more and is performed via a retropubic or perineal approach or via a minimally invasive robotic-assisted or hand-held laparoscopic approach. Outcomes can be predicted using postoperative nomograms that consider pretreatment factors and the pathologic findings at surgery. PSA failure is usually defined as a value greater than 0.1 or 0.2 ng/mL. Specific criteria to guide the choice of one approach over another are lacking. Minimally invasive approaches offer the advantage of a shorter hospital stay and reduced blood loss. Rates of cancer control, recovery of continence, and recovery of erectile function are comparable between open and minimally invasive approaches. The individual surgeon rather than the surgical approach used is most important in determining outcomes after surgery.
Neoadjuvant hormonal therapy has also been explored in an attempt to improve the outcomes of surgery for high-risk patients, using a variety of definitions. The results of several large trials testing 3 or 8 months of androgen depletion before surgery showed that serum PSA levels decreased by 96%, prostate volumes decreased by 34%, and margin positivity rates decreased from 41% to 17%. Unfortunately, hormones did not produce an improvement in PSA relapse–free survival. Thus, neoadjuvant hormonal therapy is not recommended.
Factors associated with incontinence following radical prostatectomy include older age and urethral length, which impacts the ability to preserve the urethra beyond the apex and the distal sphincter. The skill and experience of the surgeon are also factors. Recovery of erectile function is associated with younger age, quality of erections before surgery, and the absence of damage to the neurovascular bundles. In general, erectile function begins to return about 6 months after surgery if both neurovascular bundles are preserved. Potency is reduced by half if at least one neurovascular bundle is sacrificed. Overall, with the availability of drugs such as phosphodiesterase-5 (PDE5) inhibitors, intraurethral inserts of alprostadil, and intracavernosal injections of vasodilators, many patients recover satisfactory sexual function.
Radiation Therapy Radiation therapy is given by external beam, by radioactive sources implanted into the gland, or by a combination of the two techniques.
EXTERNAL-BEAM RADIATION THERAPY Contemporary external-beam radiation therapy requires three-dimensional conformal treatment plans to maximize the dose to the prostate and to minimize the exposure of the surrounding normal tissue. Intensity-modulated radiation therapy (IMRT) permits shaping of the dose and allows the delivery of higher doses to the prostate and a further reduction in normal tissue exposure than three-dimensional conformal treatment alone. These advances have enabled the safe administration of doses >80 Gy and resulted in higher local control rates and fewer side effects.
Cancer control after radiation therapy has been defined by various criteria, including a decline in PSA to <0.5 or 1 ng/mL, “nonrising” PSA values, and a negative biopsy of the prostate 2 years after completion of treatment. The current standard definition of biochemical failure (the Phoenix definition) is a rise in PSA by ≥2 ng/mL higher than the lowest PSA achieved. The date of failure is “at call” and not backdated.
Radiation dose is critical to the eradication of prostate cancer. In a representative study, a PSA nadir of <1.0 ng/mL was achieved in 90% of patients receiving 75.6 or 81.0 Gy versus 76% and 56% of those receiving 70.2 and 64.8 Gy, respectively. Positive biopsy rates at 2.5 years were 4% for those treated with 81 Gy versus 27% and 36% for those receiving 75.6 and 70.2 Gy, respectively.
Overall, radiation therapy is associated with a higher frequency of bowel complications (mainly diarrhea and proctitis) than surgery. The frequency relates directly to the volume of the anterior rectal wall receiving full-dose treatment. In one series, grade 3 rectal or urinary toxicities were seen in 2.1% of patients who received a median dose of 75.6 Gy, whereas grade 3 urethral strictures requiring dilatation developed in 1% of cases, all of whom had undergone a transurethral resection of the prostate (TURP). Pooled data show that the frequency of grade 3 and 4 toxicities is 6.9% and 3.5%, respectively, for patients who received >70 Gy. The frequency of erectile dysfunction is related to the age of the patient, the quality of erections pretreatment, the dose administered, and the time of assessment. Postradiation erectile dysfunction is related to a disruption of the vascular supply and not the nerve fibers.
Neoadjuvant hormone therapy before radiation therapy has the aim of decreasing the size of the prostate and, consequently, reducing the exposure of normal tissues to full-dose radiation, increasing local control rates, and decreasing the rate of systemic failure. Short-term hormone therapy can reduce toxicities and improve local control rates, but long-term treatment (2–3 years) is needed to prolong the time to PSA failure and lower the risk of metastatic disease in men with high-risk cancers. The impact on survival has been less clear.
BRACHYTHERAPY Brachytherapy is the direct implantation of radioactive sources (seeds) into the prostate. It is based on the principle that the deposition of radiation energy in tissues decreases as a function of the square of the distance from the source (Chap. 103e). The goal is to deliver intensive irradiation to the prostate, minimizing the exposure of the surrounding tissues. The current standard technique achieves a more homogeneous dose distribution by placing seeds according to a customized template based on imaging assessment of the cancer and computer-optimized dosimetry. The implantation is performed transperineally as an outpatient procedure with real-time imaging.
Improvements in brachytherapy techniques have resulted in fewer complications and a marked reduction in local failure rates. In a series of 197 patients followed for a median of 3 years, 5-year actuarial PSA relapse–free survival for patients with pretherapy PSA levels of 0–4, 4–10, and >10 ng/mL were 98%, 90%, and 89%, respectively. In a separate report of 201 patients who underwent posttreatment biopsies, 80% were negative, 17% were indeterminate, and 3% were positive. The results did not change with longer follow-up. Nevertheless, many physicians feel that implantation is best reserved for patients with good or intermediate prognostic features.
Brachytherapy is well tolerated, although most patients experience urinary frequency and urgency that can persist for several months. Incontinence has been seen in 2–4% of cases. Higher complication rates are observed in patients who have undergone a prior TURP, whereas those with obstructive symptoms at baseline are at a higher risk for retention and persistent voiding symptoms. Proctitis has been reported in <2% of patients.
Active Surveillance Although prostate cancer is the most common form of cancer affecting men in the United States, patients are being diagnosed earlier and more frequently present with early-stage disease. Active surveillance, described previously as watchful waiting or deferred therapy, is the policy of monitoring the illness at fixed intervals with DREs, PSA measurements, and repeat prostate biopsies as indicated until histopathologic or serologic changes correlative of progression warrant treatment with curative intent. It evolved from studies that evaluated predominantly elderly men with well-differentiated tumors who demonstrated no clinically significant progression for protracted periods, recognition of the contrast between incidence and disease-specific mortality, the high prevalence of autopsy cancers, and an effort to reduce overtreatment. A recent screening study estimated that between 50–100 men with low-risk disease would need to be treated to prevent one prostate cancer–specific death.
Arguing against active surveillance are the results of a Swedish randomized trial of radical prostatectomy versus active surveillance. With a median follow-up of 6.2 years, men treated by radical surgery had a lower risk of prostate cancer death relative to active surveillance patients (4.6% vs 8.9%) and a lower risk of metastatic progression (hazard ratio 0.63). Case selection is critical, and determining clinical parameters predictive of cancer aggressiveness that can be used to reliably select men most likely to benefit from active surveillance is an area of intense study. In one prostatectomy series, it was estimated that 10–15% of those treated had “insignificant” disease. One set of criteria includes men with clinical T1c tumors that are biopsy Gleason grade 6 or less involving three or fewer cores, each of them having less than 50% involvement by tumor and a PSA density of less than 0.15.
Concerns about active surveillance include the limited ability to predict pathologic findings by needle biopsy even when multiple cores are obtained, the recognized multifocality of the disease, and the possibility of a missed opportunity to cure the disease. Nomograms to help predict which patients can safely be managed by active surveillance continue to be refined, and as their predictive accuracy improves, it can be anticipated that more patients will be candidates.
RISING PSA AFTER DEFINITIVE LOCAL THERAPY
This term is applied to a group of patients in whom the sole manifestation of disease is a rising PSA after surgery and/or radiation therapy. By definition, there is no evidence of disease on an imaging study. For these patients, the central issue is whether the rise in PSA results from persistent disease in the primary site, systemic disease, or both. In theory, disease in the primary site may still be curable by additional local treatment.
The decision to recommend radiation therapy after prostatectomy is guided by the pathologic findings at surgery, because imaging studies such as CT and bone scan are typically uninformative. Some recommend a choline-11 positron emission tomography (PET) scan, but availability in the United States is limited. Others recommend that a biopsy of the urethrovesical anastomosis be obtained before considering radiation, whereas others treat empirically based on risk. Factors that predict for response to salvage radiation therapy are a positive surgical margin, lower Gleason score in the radical prostatectomy specimen, long interval from surgery to PSA failure, slow PSA doubling time, absence of disease in the lymph nodes, and a low (<0.5–1 ng/mL) PSA value at the time of radiation treatment. Radiation therapy is generally not recommended if the PSA was persistently elevated after surgery, which usually indicates that the disease has spread outside of the area of the prostate bed and is unlikely to be controlled with radiation therapy. As is the case for other disease states, nomograms to predict the likelihood of success are available.
For patients with a rising PSA after radiation therapy, salvage local therapy can be considered if the disease was “curable” at the time of diagnosis, if persistent disease has been documented by a biopsy of the prostate, and if no metastatic disease is seen on imaging studies. Unfortunately, case selection is poorly defined in most series, and morbidities are significant. Options include salvage radical prostatectomy, salvage cryotherapy, salvage radiation therapy, and salvage irreversible electroporation.
The rise in PSA after surgery or radiation therapy may indicate subclinical or micrometastatic disease with or without local recurrence. In these cases, the need for treatment depends, in part, on the estimated probability that the patient will develop clinically detectable metastatic disease on a scan and in what time frame. That immediate therapy is not always required was shown in a series where patients who developed a biochemical recurrence after radical prostatectomy received no systemic therapy until metastatic disease was documented. Overall, the median time to metastatic progression by imaging was 8 years, and 63% of the patients with rising PSA values remained free of metastases at 5 years. Factors associated with progression included the Gleason score of the radical prostatectomy specimen, time to recurrence, and PSA doubling time. For those with Gleason grade ≥8, the probability of metastatic progression was 37%, 51%, and 71% at 3, 5, and 7 years, respectively. If the time to recurrence was <2 years and PSA doubling time was long (>10 months), the proportions with metastatic disease at the same time intervals were 23%, 32%, and 53%, versus 47%, 69%, and 79% if the doubling time was short (<10 months). PSA doubling times are also prognostic for survival. In one series, all patients who succumbed to disease had PSA doubling times of 3 months or less.
Most physicians advise treatment if the PSA doubling time is 12 months or less. A difficulty with predicting the risk of metastatic spread, symptoms, or death from disease in the rising PSA state is that most patients receive some form of therapy before the development of metastases. Nevertheless, predictive models continue to be refined.
METASTATIC DISEASE: NONCASTRATE
The state of noncastrate metastatic prostate cancer includes men with metastases visible on an imaging study and noncastrate levels of testosterone (>150 ng/dL). The patient may be newly diagnosed or have a recurrence after treatment for localized disease. Symptoms of metastatic disease include pain from osseous spread, although many patients are asymptomatic despite extensive spread. Less common are symptoms related to marrow compromise (myelophthisis), spinal cord compression, or a coagulopathy.
Standard treatment is to deplete/lower androgens by medical or surgical means and/or to block androgen binding to the AR with antiandrogens. More than 90% of male hormones originate in the testes; <10% are synthesized in the adrenal gland. Surgical orchiectomy is the “gold standard” but is rarely used due to the availability of effective medical therapies and the more widespread use of hormones on an intermittent basis by which patients are treated for defined periods of time, following which the treatments are intentionally discontinued (discussed further below) (Fig. 115-3).
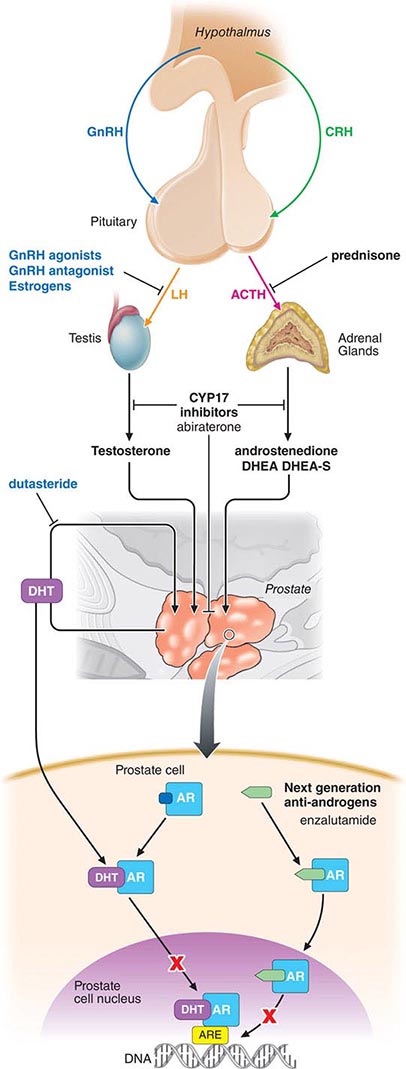
FIGURE 115-3 Sites of action of different hormone therapies. ACTH, adrenocorticotropic hormone; AR, androgen receptor; ARE, androgen-response element; CRH, corticotropin-releasing hormone; DHEA, dehydroepiandrosterone; DHEA-S, dehydroepiandrosterone sulphate; DHT, dihydrotestosterone; GnRH, gonadotropin-releasing hormone; LH, luteinizing hormone.
Testosterone-Lowering Agents Medical therapies that lower testosterone levels include the gonadotropin-releasing hormone (GnRH) agonists/antagonists, 17,20-lyase inhibitors, CYP17 inhibitors, estrogens, and progestational agents. Of these, GnRH analogues such as leuprolide acetate and goserelin acetate initially produce a rise in luteinizing hormone and follicle-stimulating hormone, followed by a downregulation of receptors in the pituitary gland, which effects a chemical castration. They were approved on the basis of randomized comparisons showing an improved safety profile (specifically, reduced cardiovascular toxicities) relative to diethylstilbestrol (DES), with equivalent potency. The initial rise in testosterone may result in a clinical flare of the disease. As such, these agents are relatively contraindicated in men with significant obstructive symptoms, cancer-related pain, or spinal cord compromise. GnRH antagonists such as degarelix achieve castrate levels of testosterone within 48 h without the initial rise in serum testosterone and do not cause a flare in the disease. Estrogens such as DES are rarely used due to the risk of vascular complications such as fluid retention, phlebitis, embolic events, and stroke. Progestational agents alone are less efficacious.
Agents that lower testosterone are associated with an androgen-depletion syndrome that includes hot flushes, weakness, fatigue, loss of libido, impotence, sarcopenia, anemia, change in personality, and depression. Changes in lipids, obesity, and insulin resistance, along with an increased risk of diabetes and cardiovascular disease, can also occur, mimicking the metabolic syndrome. A decrease in bone density may also result that worsens over time and results in an increased risk of clinical fractures. This is a particular concern, often underappreciated, for men with preexisting osteopenia secondary to hypogonadism or glucocorticoid or alcohol use. Baseline fracture risk can be assessed using the Fracture Risk Assessment Scale (FRAX), and to minimize fracture risk, patients are advised to take calcium and vitamin D supplementation, along with a bisphosphonate or the RANK ligand inhibitor, denosumab.
Antiandrogens First-generation nonsteroidal antiandrogens such as flutamide, bicalutamide, and nilutamide block ligand binding to the AR and were initially approved to block the disease flare that may occur with the rise in serum testosterone associated with GnRH agonist therapy. When antiandrogens are given alone, testosterone levels typically increase above baseline, but relative to testosterone-lowering therapies, they cause fewer hot flushes, less of an effect on libido, less muscle wasting, fewer personality changes, and less bone loss. Gynecomastia remains a significant problem but can be alleviated in part by tamoxifen.
Most reported randomized trials suggest that the cancer-specific outcomes are inferior when antiandrogens are used alone. Bicalutamide, even at 150 mg (three times the recommended dose), was associated with a shorter time to progression and inferior survival compared to surgical castration for patients with established metastatic disease. Nevertheless, some men may accept the trade-off of a potentially inferior cancer outcome for an improved quality of life.
Combined androgen blockade, the administration of an antiandrogen plus a GnRH analogue or surgical orchiectomy, and triple androgen blockade, which includes the addition of a 5ARI, have not been shown to be superior to androgen depletion monotherapies and are no longer recommended. In practice, most patients who are treated with a GnRH agonist receive an antiandrogen for the first 2–4 weeks of treatment to protect against the flare.
Intermittent Androgen Deprivation Therapy (IADT) The use of hormones in an “on-and-off” approach was initially proposed as a way to prevent the selection of cells that are resistant to androgen depletion and to reduce side effects. The hypothesis is that by allowing endogenous testosterone levels to rise, the cells that survive androgen depletion will induce a normal differentiation pathway. It is postulated that by allowing the surviving cells to proliferate in the presence of androgen, sensitivity to subsequent androgen depletion will be retained and the chance of developing a castration-resistant state will be reduced. Applied in the clinic, androgen depletion is continued for 2–6 months beyond the point of maximal response. Once treatment is stopped, endogenous testosterone levels increase, and the symptoms associated with hormone treatment abate. PSA levels also begin to rise, and at some level, treatment is restarted. With this approach, multiple cycles of regression and proliferation have been documented in individual patients. It is unknown whether the intermittent approach increases, decreases, or does not change the overall duration of sensitivity to androgen depletion. The approach is safe, but long-term data are needed to assess the course in men with low PSA levels. A randomized trial showed similar survival time between patients treated with intermittent versus continuous treatment, with a slightly higher risk of prostate cancer–specific mortality in the intermittent group, and higher cardiovascular mortality in patients on continuous therapy. The intermittent therapy was better tolerated.
Outcomes of Androgen Depletion The anti–prostate cancer effects of the various androgen depletion/blockade strategies are similar, and the outcomes predictable: an initial response, then a period of stability in which tumor cells are dormant and nonproliferative, followed after a variable period of time by a rise in PSA and tumor regrowth as a castration-resistant lesion that for most men is invariably lethal. Androgen depletion is not curative because cells that survive castration are present when the disease is first diagnosed. Considered by disease manifestation, PSA levels return to normal in 60–70% of cases, and measurable lesions regress in about 50%; improvements in bone scan occur in 25% of cases, but the majority of cases remain stable. The duration of response and survival is inversely proportional to disease extent at the time androgen depletion is first started, whereas the degree of PSA decline at 6 months has been shown to be prognostic. In a large-scale trial, PSA nadir proved prognostic.
An active question is whether hormones should be given in the adjuvant setting after surgery or radiation treatment of the primary tumor or whether to wait until PSA recurrence, metastatic disease, or symptoms are documented. Trials in support of early therapy have often been underpowered relative to the reported benefit or have been criticized on methodologic grounds. One trial showing a survival benefit for patients treated with radiation therapy and 3 years of androgen depletion, relative to radiation alone, was criticized for the poor outcomes of the control group. Another showing a survival benefit for patients with positive lymph nodes who were randomized to immediate medical or surgical castration compared to observation (p = .02) was criticized because the confidence intervals around the 5- and 8-year survival distributions for the two groups overlapped. A large randomized study comparing early to late hormone treatment (orchiectomy or GnRH analogue) in patients with locally advanced or asymptomatic metastatic disease showed that patients treated early were less likely to progress from M0 to M1 disease, to develop pain, and to die of prostate cancer. This trial was criticized because therapy was delayed “too long” in the late-treatment group. Noteworthy is that the American Society of Clinical Oncology Guidelines recommend deferring treatment until the disease has recurred and the prognosis has been reassessed. These guidelines do not support immediate therapy.
METASTATIC DISEASE: CASTRATE
Castration-resistant prostate cancer (CRPC) is defined as disease that progresses despite androgen suppression by medical or surgical therapies where the measured levels of testosterone are 50 ng/mL or lower. The rise in PSA indicates continued signaling through the AR signaling axis, the result of a series of oncogenic changes that include overexpression of androgen biosynthetic enzymes that can lead to increased intratumoral androgens, and overexpression of the receptor itself that enables signaling to occur even in the setting of low levels of androgen. The majority of CRPC cases are not “hormone-refractory,” and considering them as such can deny patients safe and effective treatment. CRPC can manifest in many ways. For some, it is a rise in PSA with no change in radiographs and no new symptoms. In others, it is a rising PSA and progression in bone with or without symptoms of disease. Still others will show soft tissue disease with or without osseous metastases, and others have visceral spread.
For the individual patient, it is first essential to ensure that a castrate status be documented. Patients receiving an antiandrogen alone, whose serum testosterone levels are elevated, should be treated first with a GnRH analogue or orchiectomy and observed for response. Patients on an antiandrogen in combination with a GnRH analogue should have the antiandrogen discontinued, because approximately 20% will respond to the selective discontinuation of the antiandrogen.
Chemotherapy and New Agents Through 2009, docetaxel was the only systemic therapy proven to prolong life. As a single agent, the drug produced PSA declines in 50% of patients, measurable disease regression in 25%, and improvement in both preexisting pain and prevention of future cancer-related pain. Since then, six agents with diverse mechanisms of action that target the tumor itself or other aspects of the metastatic process have been proven to prolong life and were FDA approved. The first was sipuleucel-T, the first biologic approach shown to prolong life in which antigen-presenting cells are activated ex vivo, pulsed with antigen, and reinfused. The second, cabazitaxel, a non–cross-resistant taxane, was shown to be superior to mitoxantrone in the post-docetaxel setting. This was followed by the CYP17 inhibitor abiraterone acetate, which lowers androgen levels in the tumor, adrenal glands, and testis, and the next-generation antiandrogen enzalutamide, which not only has a higher binding affinity to the AR relative to first-generation compounds, but uniquely inhibits nuclear location and DNA binding of the receptor complex. Both abiraterone acetate and enzalutamide were first approved for postchemotherapy treated patients on the basis of placebo-controlled phase III trials—a further indication that these tumors are not uniformly hormone-refractory. The indication for abiraterone acetate was later expanded to the prechemotherapy setting, based on a second trial using a co-primary endpoint of radiographic progression–free survival and overall survival. Similar results were seen with enzalutamide, for which an expanded indication is also anticipated. Alpharadin (radium-223 chloride), an alpha-emitting bone-seeking radioisotope, has been shown to prolong life in patients with symptoms related to osseous disease. The alpharadin result validated the bone microenvironment as a therapeutic target independent of direct effects on the tumor itself, as no declines in PSA were observed in the trial. Notable is that in addition to a survival benefit, the drug also reduced the development of significant skeletal events.
Other bone-targeted agents, such as the bisphosphonates and the RANK ligand inhibitor denosumab, protect against bone loss associated with androgen depletion and also reduce skeletal-related events by targeting bone osteoclasts. In one trial, denosumab was shown to be superior to zoledronic acid with respect to skeletal-related events, but had a slightly higher frequency of osteonecrosis of the jaw.
In clinical practice, most men seek to avoid chemotherapy and are first treated with a biologic agent and/or newer hormonal agent approved for this indication. It is crucial to the management of the individual patient to define therapeutic objectives before initiating treatment, as there are defined standards of care for different disease manifestations. For example, sipuleucel-T is not indicated for patients with symptoms or visceral disease because the effects on the disease occur late. Similarly, alpharadin is not indicated for patients with disease that is predominantly in soft tissue or who have osseous disease that is not causing symptoms.
Pain Management Management of pain secondary to osseous metastatic disease is a critical part of therapy. Optimal palliation requires assessing whether the symptoms are from metastases that threaten or that are already affecting the spinal cord, the cauda equina, or the base of the skull, which are best treated with external-beam radiation, as are single sites of pain. Neurologic symptoms require emergency evaluation because loss of function may be permanent if not addressed quickly. Because the disease is often diffuse, palliation at one site is often followed by the emergence of symptoms in a separate site that had not received radiation. In these cases, bone-seeking radioisotopes such as alpharadin or the beta emitter 153Sm-EDTMP (Quadramet) can be considered in addition to abiraterone acetate, docetaxel, and mitoxantrone, each of which is formally approved for the palliation of pain due to prostate cancer metastases.
BENIGN DISEASE
BENIGN PROSTATIC HYPERTROPHY
BPH is a pathologic process that contributes to the development of lower urinary tract symptoms in men. Such symptoms, arising from lower urinary tract dysfunction, are further subdivided into obstructive symptoms (urinary hesitancy, straining, weak stream, terminal dribbling, prolonged voiding, incomplete emptying) and irritative symptoms (urinary frequency, urgency, nocturia, urge incontinence, small voided volumes). Lower urinary tract symptoms and other sequelae of BPH are not just due to a mass effect, but are also likely due to a combination of the prostatic enlargement and age-related detrusor dysfunction.
TREATMENT BENIGN PROSTATIC HYPERTROPHY
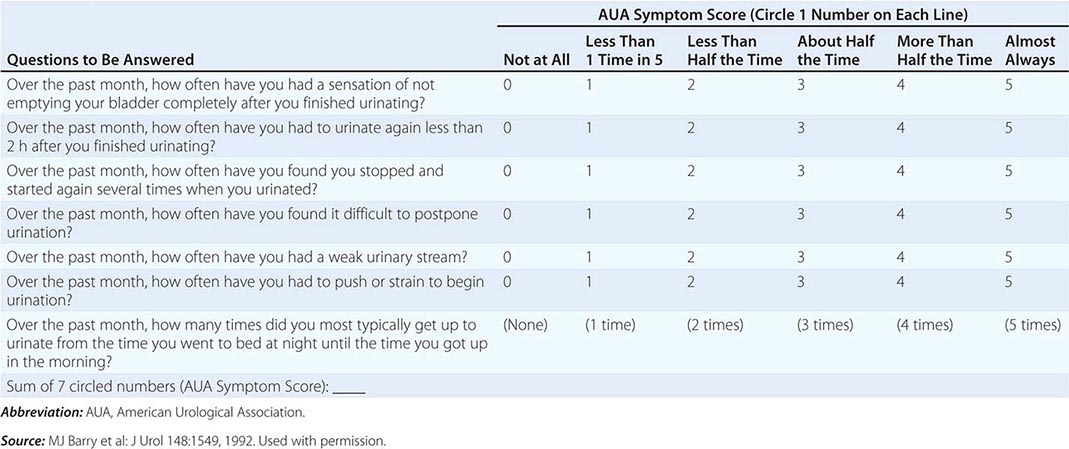
The symptoms are generally measured using a validated, reproducible index that is designed to determine disease severity and response to therapy—the AUA’s Symptom Index (AUASI), also adopted as the International Prostate Symptom Score (IPSS) (Table 115–2). Serial AUASI is particularly useful in following patients as they are treated with various forms of therapy. Asymptomatic patients do not require treatment regardless of the size of the gland, whereas patients with an inability to urinate, gross hematuria, recurrent infection, or bladder stones may require surgery. In patients with symptoms, uroflowmetry can identify those with normal flow rates who are unlikely to benefit from treatment, and bladder ultrasound can identify those with high postvoid residuals who may need intervention. Pressure-flow (urodynamic) studies detect primary bladder dysfunction. Cystoscopy is recommended if hematuria is documented and to assess the urinary outflow tract before surgery. Imaging of the upper tracts is advised for patients with hematuria, a history of calculi, or prior urinary tract problems.
AUA SYMPTOM INDEX |
Symptomatic relief is the most common reason men seek treatment for BPH, and therefore the goal of therapy for BPH is usually relief of these symptoms. Alpha-adrenergic receptor antagonists are thought to treat the dynamic aspect of BPH by reducing sympathetic tone of the bladder outlet, thereby decreasing resistance and improving urinary flow. 5ARIs are thought to treat the static aspect of BPH by reducing prostate volume and having a similar, albeit delayed effect. They have also proven to be beneficial in the prevention of BPH progression, as measured by prostate volume, the risk of developing acute urinary retention, and the risk of having BPH-related surgery. The use of an alpha-adrenergic receptor antagonist and a 5ARI as combination therapy seeks to provide symptomatic relief while preventing progression of BPH.
Another class of medications that has shown improvement in lower urinary tract symptoms secondary to BPH is PDE5 inhibitors, used currently in the treatment of erectile dysfunction. All three of the PDE5 inhibitors available in the United States, sildenafil, vardenafil, and tadalafil, appear to be effective in the treatment of symptoms secondary to BPH. The use of PDE5 inhibitors is not without controversy, however, given the fact that short-acting phosphodiesterase inhibitors such as sildenafil need to be dosed separately from alpha blockers such as tamsulosin because of potential hypotensive effects. Newer classes of pharmacologic agents have been used to treat symptoms secondary to BPH. Symptoms due to BPH often coexist with symptoms due to overactive bladder, and the most common pharmacologic agents for the treatment of overactive bladder symptoms are anticholinergics. This has led to multiple studies evaluating the efficacy of anticholinergics for the treatment of lower urinary tract symptoms secondary to BPH. Surgical therapy is now considered second-line therapy and is usually reserved for patients after a trial of medical therapy. The goal of surgical therapy is to reduce the size of the prostate, effectively reducing resistance to urine flow.
Surgical approaches include TURP, transurethral incision, or removal of the gland via a retropubic, suprapubic, or perineal approach. Also used are transurethral ultrasound-guided laser-induced prostatectomy (TULIP), stents, and hyperthermia.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


