Chapter 38 Pharmacologic management of gout relies on the use of NSAIDs (see Chapter 36), colchicine, uricosuric agents (probenecid), and xanthine oxidase inhibitors (allopurinol and febuxostat) (Table 38-1). TABLE 38-1 Pharmacologic Management of Different Phases of Gout Modified from Schlesinger N: Management of acute and chronic gouty arthritis: present state-of-the art, Drugs 64(21):2399-2416, 2004; Morgan L: Colchicine in acute gout, Aust Fam Physician 37(3):103, 2008. Use the following three mechanisms in the treatment of gout (Figure 38-1): 1. Increase the excretion of uric acid (uricosurics). 2. Decrease the synthesis of uric acid (allopurinol and febuxostat). 3. Decrease or stop the inflammatory response (NSAIDs, colchicine). NSAIDs inhibit prostaglandin synthesis, thereby reducing the intensity of inflammation and pain in injured tissue. See Chapter 34 for a detailed discussion of prostaglandin inhibition. • American College of Rheumatology, Guidelines for the management of Gout. Available at http://www.rheumatology.org/practice/clinical/guidelines/gout.asp. Released in late 2012. • Gout treatment should be individualized and guided by principles of pharmacology. • The ACR guidelines recommend xanthine oxidase inhibitors, either allopurinol or febuxostat, as first-line therapy to reduce uric acid levels. • A uricosuric agent such as probenecid, fenofibrate or losartan can be added if the target serum urate level cannot be achieved with xanthine oxidase inhibitors alone. • Treatment should be titrated to achieve a serum urate level of less than 6 mg/dl, but a reduction to 5 mg/dl might be needed to control signs and symptoms. • Consider select pharmacogenetic screening of patients for the HLA-B∗5801 allele, which increases the risk of allopurinol hypersensitivity in high-risk populations, including Han Chinese.
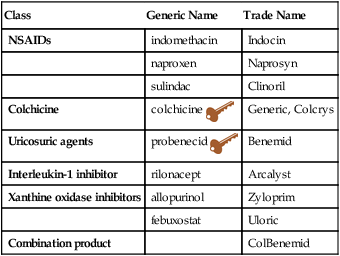
Gout Medications
Class
Generic Name
Trade Name
NSAIDs
indomethacin
Indocin
naproxen
Naprosyn
sulindac
Clinoril
Colchicine
colchicine 
Generic, Colcrys
Uricosuric agents
probenecid 
Benemid
Interleukin-1 inhibitor
rilonacept
Arcalyst
Xanthine oxidase inhibitors
allopurinol
Zyloprim
febuxostat
Uloric
Combination product
ColBenemid
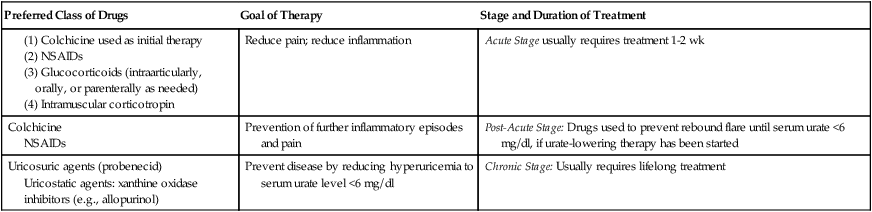
Preferred Class of Drugs
Goal of Therapy
Stage and Duration of Treatment
Reduce pain; reduce inflammation
Acute Stage usually requires treatment 1-2 wk
Colchicine
NSAIDs
Prevention of further inflammatory episodes and pain
Post-Acute Stage: Drugs used to prevent rebound flare until serum urate <6 mg/dl, if urate-lowering therapy has been started
Uricosuric agents (probenecid)
Uricostatic agents: xanthine oxidase inhibitors (e.g., allopurinol)
Prevent disease by reducing hyperuricemia to serum urate level <6 mg/dl
Chronic Stage: Usually requires lifelong treatment
Mechanism of Action
Treatment Principles
Standardized Guidelines
Cardinal Points of Treatment
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Gout Medications

 Key drug. Drugs are listed in approximate order of use.
Key drug. Drugs are listed in approximate order of use.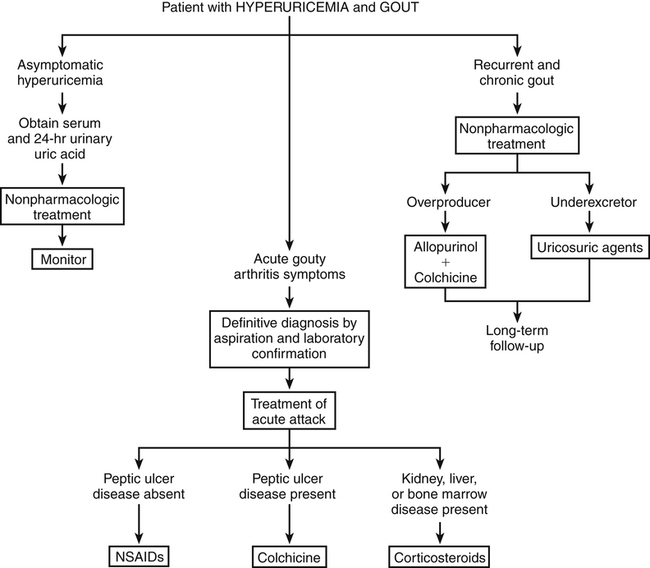
Only gold members can continue reading. Log In or Register to continue
