Chapter 1 General Appearance, Facies, and Body Habitus
General Appearance
2 Which aspects of the patient should be assessed?



 Body habitus and body proportions
Body habitus and body proportions



 Alertness and state of consciousness
Alertness and state of consciousness
 Degree of illness, whether acute or chronic
Degree of illness, whether acute or chronic



A. Posture
3 What information can be obtained from observing the patient’s posture?
In abdominal pain the posture is often so typical as to localize the disease:
 Patients with pancreatitis usually lie in the fetal position: on one side, with knees and legs bent over.
Patients with pancreatitis usually lie in the fetal position: on one side, with knees and legs bent over.
 Patients with peritonitis are very still and avoid any movement that might worsen the pain.
Patients with peritonitis are very still and avoid any movement that might worsen the pain.
 Patients with intestinal obstruction are instead quite restless.
Patients with intestinal obstruction are instead quite restless.
 Patients with renal or perirenal abscesses bend toward the side of the lesion.
Patients with renal or perirenal abscesses bend toward the side of the lesion.


 Patients with a large pleural effusion tend to lie on the affected side to maximize excursions of the unaffected side. This, however, worsens hypoxemia (see Chapter 13, questions 48–51).
Patients with a large pleural effusion tend to lie on the affected side to maximize excursions of the unaffected side. This, however, worsens hypoxemia (see Chapter 13, questions 48–51).



4 What is the posture of patients with dyspnea?
An informative alphabet soup of orthopnea, paroxysmal nocturnal dyspnea, platypnea and orthodeoxia, trepopnea, respiratory alternans, and abdominal paradox. These can determine not only the severity of dyspnea, but also its etiology (see Chapter 13, questions 35–51).
B. State of Hydration
5 What is hypovolemia?
A condition characterized by volume depletion and dehydration:
 Volume depletion is a loss in extracellular salt, through either kidneys (diuresis) or the gastrointestinal tract (hemorrhage, vomiting, diarrhea). This causes contraction of the total intravascular pool of plasma, which results in circulatory instability and thus an increase in the serum urea nitrogen-to-creatinine ratio—a valuable biochemical marker for volume depletion.
Volume depletion is a loss in extracellular salt, through either kidneys (diuresis) or the gastrointestinal tract (hemorrhage, vomiting, diarrhea). This causes contraction of the total intravascular pool of plasma, which results in circulatory instability and thus an increase in the serum urea nitrogen-to-creatinine ratio—a valuable biochemical marker for volume depletion.



9 How do you determine the presence of hypovolemia?
Through the “tilt test,” which measures postural changes in heart rate and blood pressure (BP):
1. Ask the patient to lie supine.
3. Measure heart rate and blood pressure in this position.
6. Measure heart rate and then blood pressure while the patient is standing. Measure rate by counting over 30 seconds and multiplying by two, which is more accurate than counting over 15 seconds and multiplying by four.
12 Should the patient lie supine for more than 2 minutes before standing up?
No. A longer period does not increase the sensitivity of the test.
14 What is the normal response to the tilt test?
Going from supine to standing, a normal patient exhibits the following:
 Heart rate increases by 10.9 ± 2 beats/minute and usually stabilizes after 45–60 seconds.
Heart rate increases by 10.9 ± 2 beats/minute and usually stabilizes after 45–60 seconds.
 Systolic blood pressure decreases only slightly (by 3.5 ± 2 mmHg) and stabilizes in 1–2 minutes.
Systolic blood pressure decreases only slightly (by 3.5 ± 2 mmHg) and stabilizes in 1–2 minutes.
 Diastolic blood pressure increases by 5.2 ± 2.4 mmHg. This, too, stabilizes within 1–2 minutes.
Diastolic blood pressure increases by 5.2 ± 2.4 mmHg. This, too, stabilizes within 1–2 minutes.
18 So what are the findings of a positive tilt test for hypovolemia?
 The most helpful is a postural increase in heart rate of at least 30 beats/minute (which has a sensitivity of 97% and a specificity of 96% for blood loss >630 mL). This change (as well as severe postural dizziness, see later) may last 12–72 hours if IV fluids are not administered.
The most helpful is a postural increase in heart rate of at least 30 beats/minute (which has a sensitivity of 97% and a specificity of 96% for blood loss >630 mL). This change (as well as severe postural dizziness, see later) may last 12–72 hours if IV fluids are not administered.







29 What is the significance of dry mucous membranes in children?



C. State of Nutrition
33 Why is the BMI important?
Because a high BMI is associated with increased risk for serious medical problems:










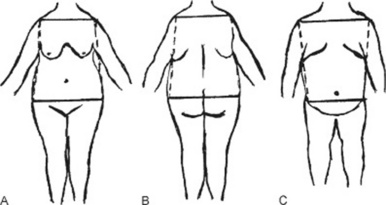
38 How important is the distribution of body fat?
Very important, since it strongly determines the impact of obesity on health. Fat deposition may be central (mostly in the trunk) or peripheral (mostly in the extremities) (Fig. 1-1).
 Central obesity has a bihumeral diameter greater than the bitrochanteric diameter; subcutaneous fat has a “descending” distribution, being mostly concentrated in the upper half of the body (neck, cheeks, shoulder, chest, and upper abdomen).
Central obesity has a bihumeral diameter greater than the bitrochanteric diameter; subcutaneous fat has a “descending” distribution, being mostly concentrated in the upper half of the body (neck, cheeks, shoulder, chest, and upper abdomen).

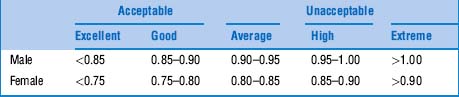
42 What is the WHR threshold for cardiovascular risk?
The cutoff seems to be a waist-to-hip ratio of 0.83 for women and 0.9 for men. Favoring WHR over BMI would result in a threefold increase in the population at risk for myocardial infarction. This would be especially valuable in Asia, where obesity by BMI is rare, but WHRs can be quite abnormal (Table 1-1).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


