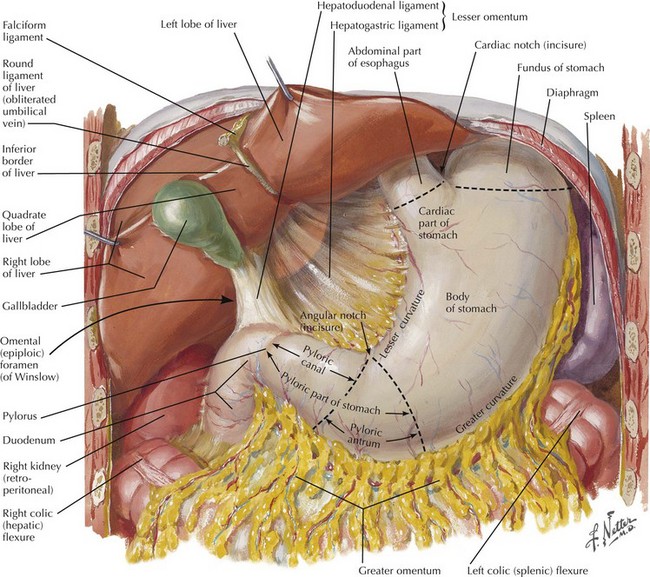
Chapter 8 The abdomen is explored to evaluate for metastatic disease, usually through an upper midline incision, although some surgeons prefer a chevron incision. Laparoscopic-assisted approaches to gastric resection are increasingly used. Figure 8-1 shows the stomach in situ with its relationship to surrounding structures. Figures 8-1, 8-2, and 8-3, A, show the arterial and venous anatomy pertinent to gastric resection.
Gastrectomy
Surgical Approach for Gastrectomy
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine