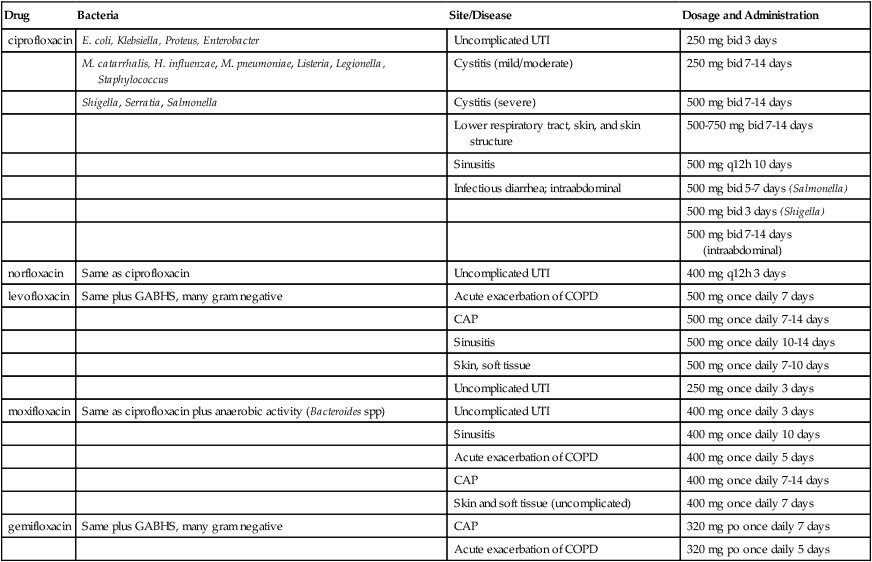
Chapter 63 INDICATIONS See Table 63-1 for specifics. TABLE 63-1 Fluoroquinolone Indications with Dosages and Recommendations CAP, Community-acquired pneumonia; GABHS, group A β-hemolytic Streptococcus pyogenes. • Monitor renal, hepatic, and hematopoietic function during prolonged therapy. • Patients on warfarin anticoagulation should be monitored closely for prothrombin times and INR at baseline—daily for the first week of therapy, and weekly thereafter. The patient should be instructed to report immediately any sign of bleeding. • Patients on any theophylline product (e.g., theophylline, oxtriphylline, aminophylline) should have serum theophylline levels monitored because theophylline clearance may be decreased with concomitant fluoroquinolone use. • Evaluate renal and hepatic function at baseline and every 6 weeks if therapy is to be continued. • Monitor hematology parameters periodically for evidence of leukopenia, hemolytic anemia, and thrombocytopenia. • Monitor for CNS side effects such as headache, weakness, shaking, dizziness, drowsiness, and confusion.
Fluoroquinolones
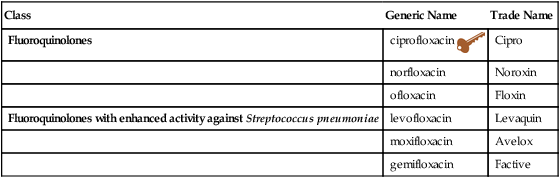
Class
Generic Name
Trade Name
Fluoroquinolones
ciprofloxacin 
Cipro
norfloxacin
Noroxin
ofloxacin
Floxin
Fluoroquinolones with enhanced activity against Streptococcus pneumoniae
levofloxacin
Levaquin
moxifloxacin
Avelox
gemifloxacin
Factive
Drug
Bacteria
Site/Disease
Dosage and Administration
ciprofloxacin
E. coli, Klebsiella, Proteus, Enterobacter
Uncomplicated UTI
250 mg bid 3 days
M. catarrhalis, H. influenzae, M. pneumoniae, Listeria, Legionella, Staphylococcus
Cystitis (mild/moderate)
250 mg bid 7-14 days
Shigella, Serratia, Salmonella
Cystitis (severe)
500 mg bid 7-14 days
Lower respiratory tract, skin, and skin structure
500-750 mg bid 7-14 days
Sinusitis
500 mg q12h 10 days
Infectious diarrhea; intraabdominal
500 mg bid 5-7 days (Salmonella)
500 mg bid 3 days (Shigella)
500 mg bid 7-14 days (intraabdominal)
norfloxacin
Same as ciprofloxacin
Uncomplicated UTI
400 mg q12h 3 days
levofloxacin
Same plus GABHS, many gram negative
Acute exacerbation of COPD
500 mg once daily 7 days
CAP
500 mg once daily 7-14 days
Sinusitis
500 mg once daily 10-14 days
Skin, soft tissue
500 mg once daily 7-10 days
Uncomplicated UTI
250 mg once daily 3 days
moxifloxacin
Same as ciprofloxacin plus anaerobic activity (Bacteroides spp)
Uncomplicated UTI
400 mg once daily 3 days
Sinusitis
400 mg once daily 10 days
Acute exacerbation of COPD
400 mg once daily 5 days
CAP
400 mg once daily 7-14 days
Skin and soft tissue (uncomplicated)
400 mg once daily 7 days
gemifloxacin
Same plus GABHS, many gram negative
CAP
320 mg po once daily 7 days
Acute exacerbation of COPD
320 mg po once daily 5 days
Treatment Principles
How to Monitor
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Fluoroquinolones

 Key drug.
Key drug.Only gold members can continue reading. Log In or Register to continue
