Fat Necrosis
Key Facts
Terminology
Common benign inflammatory reaction secondary to injury of breast adipose tissue
Wide spectrum of clinical and radiologic appearances
May be confused with carcinoma, both clinically and radiologically
Etiology/Pathogenesis
May be due to trauma, surgical procedures, pressure necrosis, radiation, or other rare causes
Image Findings
Reflect histological evolution of inflammatory process
Common findings are dystrophic calcifications and radiolucent oil cysts
Oil cysts may be associated with continuous eggshell calcification
Irregular mass may be present
Microscopic Pathology
Early changes: Hemorrhage in fat with induration
Followed by cystic degeneration with oily fluid secondary to necrotic fat
Calcifications frequently develop in cyst wall
Later changes: Hemosiderin deposition, varying degrees of fibrosis and calcification
Top Differential Diagnoses
Granular cell tumor
Other inflammatory lesions
Lupus mastitis
Erdheim-Chester disease
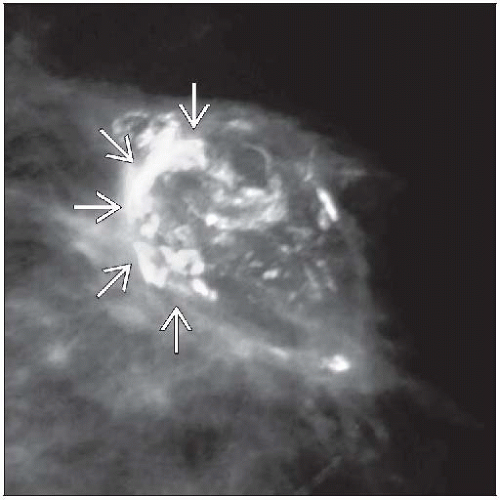 Calcifications around the edge of a central area of fat necrosis gives rise to a characteristic eggshell appearance  radiographically. Fewer calcifications can appear as a suspicious cluster. radiographically. Fewer calcifications can appear as a suspicious cluster. |
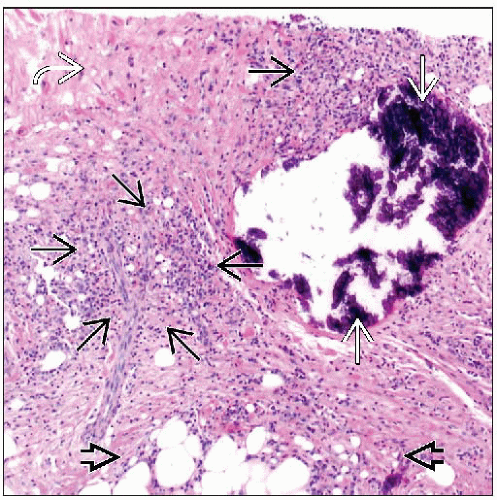 Fat necrosis includes a histiocytic infiltrate reacting to degenerating adipose tissue  with varying amounts of lymphocytic infiltrates with varying amounts of lymphocytic infiltrates  , fibrosis , fibrosis  , and calcifications , and calcifications  . . |
TERMINOLOGY
Abbreviations
Fat necrosis (FN)
Definitions
Common benign inflammatory reaction that is secondary to injury of breast connective tissue and adipose tissue
ETIOLOGY/PATHOGENESIS
Causes of Fat Necrosis
Trauma
Blunt trauma to breast
Seat belt injury after motor vehicle crashes
Produces different radiologic patterns of injury in driver and passenger
Pressure necrosis
Can occur in lower portion of pendulous breasts
Radiation therapy
Post-radiation vascular damage (endarteritis obliterans) with subsequent ischemia
Surgery
Cyst aspiration
Core needle biopsies
Excisions
Reduction mammoplasty
Implants
Autologous fat injection
Other rare causes
Polyarteritis nodosa, Weber-Christian disease, granulomatous angiopanniculitis
Heparin-induced thrombocytopenia (single case report)
In about 50% of patients, cause is unknown
CLINICAL ISSUES
Epidemiology
Incidence
Estimated to be 0.6% of breast excisions
Age
Broad range: 37-68 years (mean: ˜ 50 years)
Presentation
Symptomatic FN typically presents as palpable mass
May enlarge, remain unchanged, regress, or resolve
FN is typically detected in periareolar area and is often superficial in location
These sites are most vulnerable to trauma
Can be associated with skin changes
Bruising and tenderness (due to original trauma)
Skin tethering or dimpling, nipple retraction (due to fibrosis associated with healing)
May be detected on mammographic screening
Forms multiple types of lesions
Lipid cysts, coarse calcifications, focal asymmetries, microcalcifications, or irregular masses
Many cases can be identified by radiographic appearance
Biopsy is required for cases with unusual imaging features
Prognosis
Benign inflammatory process that should regress or resolve over time
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


