http://evolve.elsevier.com/McCuistion/pharmacology/
Drugs for Disorders of the Eye
Problems associated with the eyes may occur as the result of injuries, infections, or specific noninfectious eye disorders such as glaucoma and macular degeneration. Most drugs used to treat these conditions are topical medications in formulations developed specifically for eyes. Drugs designed to be applied to the eyes are known as ocular or ophthalmic drugs.
Diagnostic Stains
Diagnostic stains (Table 44.1) are frequently used to locate extraocular lesions or foreign objects, evaluate dry eyes, or evaluate extraocular changes. Stains may be combined with local anesthetics to allow examination that is more thorough by alleviating pain associated with the examination. Patients should be informed that these drugs will cause discoloring of the external eye and will dissipate over several hours; they may also stain nasal secretions if the lacrimal ducts (tear ducts) are patent, and they discolor soft contact lenses. Contact lenses should be removed before administration, and the eye should be rinsed with sterile normal saline solution after the procedure. Contact lenses can be replaced after 1 hour.
TABLE 44.1
Diagnostic Stains for Eye Disorders
| Diagnostic Aid | Purpose |
| Fluorescein sodium, ophthalmic | Stains the anterior segment of the eye to visualize the anterior ocular surface for defects and for contact lens fitting. When viewed through the cobalt blue filter of the ophthalmoscope or under a Wood lamp, corneal scratches and lesions fluoresce a bright yellow green. |
| Rose bengal, ophthalmic | Stains the anterior segment of the eye to visualize defects or dry eye.Defective and normal cells are stained a pink-violet color.Staining of normal cells and stinging and mild tissue toxicity limit use. |
| Lissamine green | Stains the anterior segment of the eye to visualize defects and dry eyes.Defective cells are stained green. |
Topical Anesthetics
Topical anesthetics are used in selected aspects of a comprehensive eye examination and in a variety of ophthalmic procedures. Ophthalmic anesthetics act by locally blocking the pain signals at the eye’s nerve endings. The two most common topical ophthalmic anesthetics are proparacaine hydrochloride (HCl) and tetracaine HCl. Both medications, available in solutions, are administered as drops. Ophthalmic anesthetics should be administered by a trained clinician.
Corneal anesthesia usually starts occurring within 15 seconds and lasts about 15 minutes. The blink reflex is temporarily lost, therefore the corneal epithelium may become dry. Protecting the eye from irritating chemicals, foreign bodies, and corneal scratches is important. The patient must be instructed that the affected eye will be insensitive to touch and to not rub, touch, or wipe the affected eye. Contact lenses may be reinserted after the anesthetic has completely worn off, usually after 20 minutes.
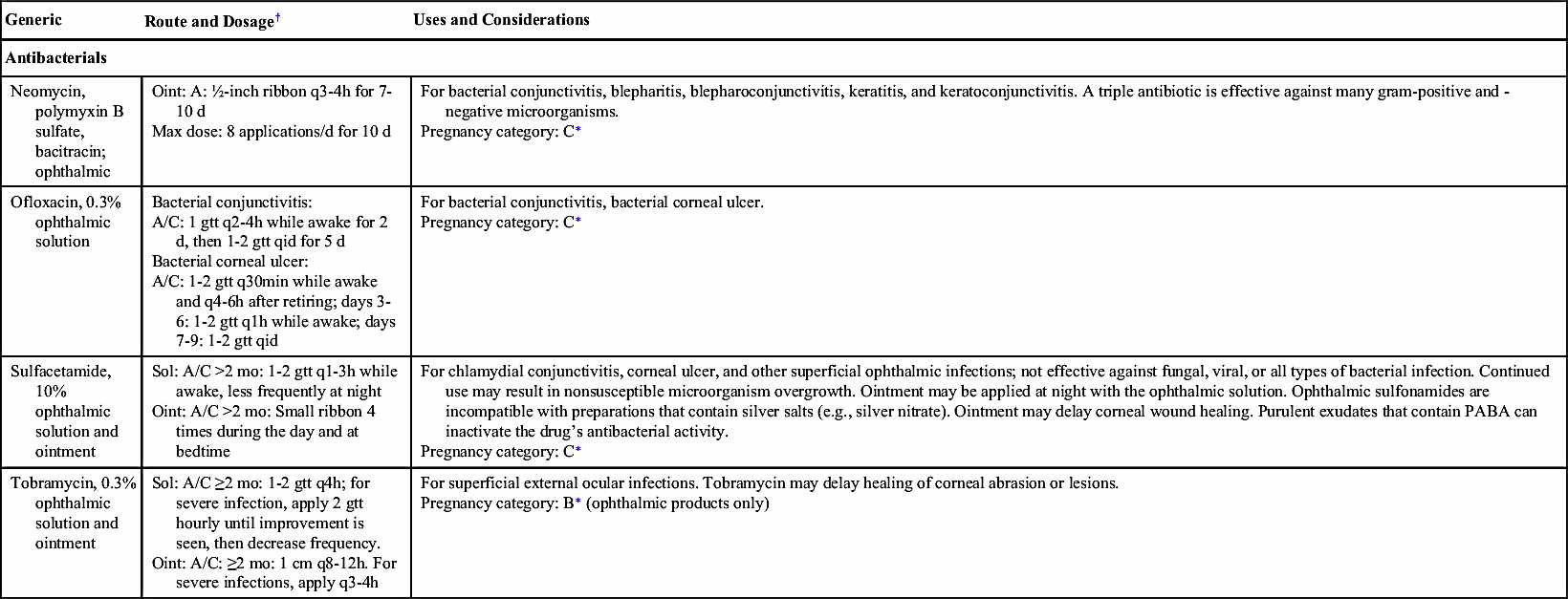
Antiinfectives
Antiinfectives (Table 44.2) are frequently used for eye infections. Conjunctivitis, an inflammation of the membrane (conjunctiva) covering the eye and inner eyelids, is the most common eye condition. Conjunctivitis is also called “pink eye” and can occur because of bacteria, viruses, and allergens. Bacterial conjunctivitis usually requires antiinfective therapy to either kill or inhibit the spread of bacteria. Some ocular viral infections (e.g., cytomegalovirus [CMV] and herpes simplex virus [HSV]) may require antiviral therapy. Examples of other ocular conditions caused by pathogens treated with ophthalmic antiinfective drugs include the following:
• Blepharitis, infection of the margins of the eyelid
• Chalazion, infection of the meibomian glands of the eyelids that may produce cysts, causing blockage of the ducts
• Bacterial and fungal endophthalmitis, infection and inflammation of structures of the inner eye
• Hordeolum, a local infection of eyelash follicles and glands on lid margins, also known as a stye
• Infectious keratitis, corneal infection and inflammation
• Infectious uveitis, infection of the vascular layer of the eye (ciliary body, choroid, and iris)
Before administering ophthalmic antiinfectives, the nurse should screen the patient for previous allergic reactions. Noninfectious conjunctivitis and local skin and eye irritation are possible side effects of ophthalmic antiinfective drugs.
Antiinflammatories
Inflammatory conditions of the eye not related to infectious pathogens often require treatment with antiinflammatory drugs (Table 44.3). If the inflammation is secondary to a bacterial or fungal infection, an antibiotic or antifungal agent is included in the medication regimen. Some ocular antiinflammatories are combined with antibacterials. Many antiinflammatories are not appropriate in patients with ocular viral infections.
Inflammation associated with keratoconjunctivitis sicca, causing lymphocytes to damage the lacrimal gland, results in fibrosis and loss of tear production; this can lead to xerophthalmia (dry eyes). Immunomodulators, such as cyclosporine ophthalmic emulsion, is an immunosuppressant that relieves xerophthalmia by a mechanism that is different from over-the-counter (OTC) lubricants. Ophthalmic cyclosporine acts as a partial immunomodulatory that causes apoptosis of lymphocytes and allows tear production to resume.
Ophthalmic nonsteroidal antiinflammatory drugs (NSAIDs) such as diclofenac sodium and ketorolac tromethamine inhibit miosis by preventing the formation of ocular prostaglandins. Most of these drugs are used for management or prevention of ocular inflammation before and following eye surgery. Unlike corticosteroids, NSAIDs do not affect intraocular pressure (IOP) (IOP is further discussed in Glaucoma and Ocular Hypertension Drugs). However, ocular NSAIDs can increase bleeding tendencies and delay corneal healing. Topical NSAIDs are not expected to increase cardiovascular risk, hepatic reactions, or other systemic adverse effects; however, ocular NSAIDs can cause bleeding of ocular tissues.
Ophthalmic corticosteroids such as dexamethasone and prednisolone acetate are another type of antiinflammatory. Corticosteroids are used to treat a number of eye conditions, such as allergic conjunctivitis, herpes zoster keratitis (not herpes simplex keratitis), corneal abrasion, postoperative ocular inflammation, and optic neuritis.  Ocular corticosteroids can mask infections and delay healing and are contraindicated in persons with untreated ocular infections. Corticosteroids can worsen glaucoma by reducing the outflow of aqueous humor and increasing IOP; the effects are usually reversible upon discontinuation of the drug. Prolonged use can cause open-angle glaucoma, ocular nerve damage, or visual defects. Refer to Chapter 24 for more information on corticosteroids.
Ocular corticosteroids can mask infections and delay healing and are contraindicated in persons with untreated ocular infections. Corticosteroids can worsen glaucoma by reducing the outflow of aqueous humor and increasing IOP; the effects are usually reversible upon discontinuation of the drug. Prolonged use can cause open-angle glaucoma, ocular nerve damage, or visual defects. Refer to Chapter 24 for more information on corticosteroids.
Ocular corticosteroids can mask infections and delay healing and are contraindicated in persons with untreated ocular infections. Corticosteroids can worsen glaucoma by reducing the outflow of aqueous humor and increasing IOP; the effects are usually reversible upon discontinuation of the drug. Prolonged use can cause open-angle glaucoma, ocular nerve damage, or visual defects. Refer to Chapter 24 for more information on corticosteroids.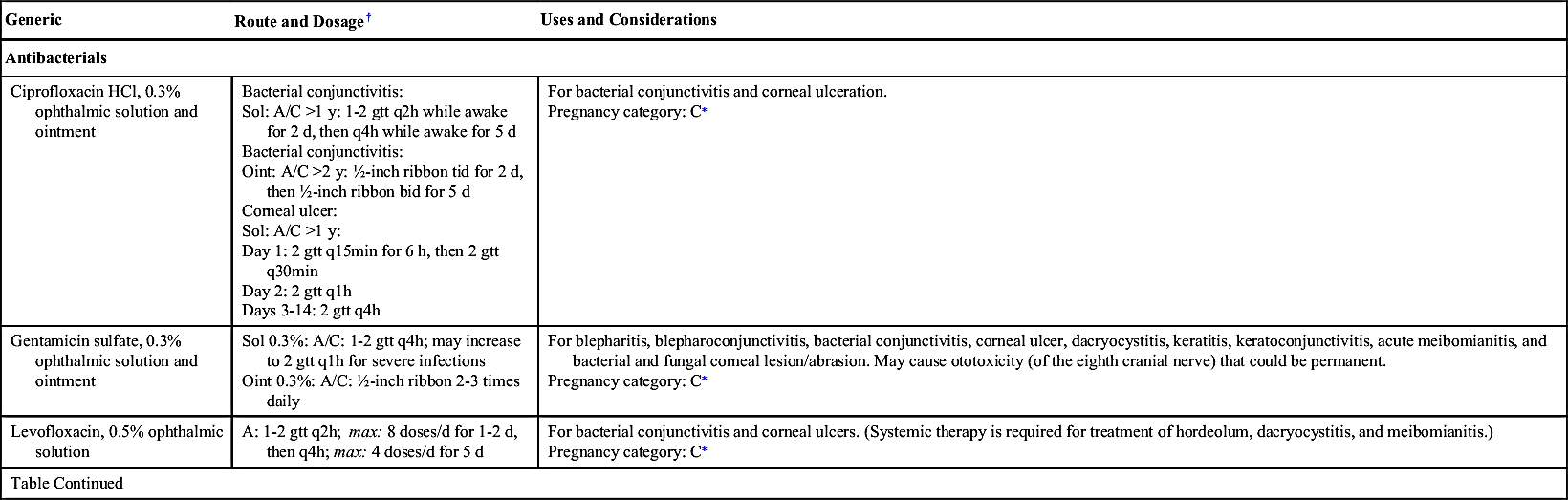



When allergies are the cause of eye inflammation, ophthalmic allergy drugs are commonly prescribed to treat the underlying cause. These allergy drugs contain antihistamines and mast cell stabilizers. Antihistamines block histamine from activating histamine receptors in the tissues. Degranulation of mast cells releases histamine and other inflammatory mediators; mast cell stabilizers prevent mast cells from degranulating. Ocular sensations that include burning, stinging, and blurred vision are common adverse effects reported. Other adverse effects include cephalgia, dysgeusia, and rhinitis.
Decongestants
Eye inflammation typically presents with redness due to vascular congestion of the conjunctiva. Ophthalmic decongestants such as phenylephrine, naphazoline, and tetrahydrozoline stimulate alpha-adrenergic receptors in the arterioles of the conjunctiva, vasoconstricting (narrowing) the blood vessels and thereby decreasing congestion. Many ocular decongestants are available without prescription. If these are absorbed in significant amounts, their sympathetic nervous system effects may pose problems for patients with increased IOP and hypertension.  Ocular decongestants are contraindicated in patients with angle-closure glaucoma because these drugs may contribute to acute angle-closure, a medical emergency.
Ocular decongestants are contraindicated in patients with angle-closure glaucoma because these drugs may contribute to acute angle-closure, a medical emergency.
Ocular decongestants are contraindicated in patients with angle-closure glaucoma because these drugs may contribute to acute angle-closure, a medical emergency.Lubricants
Eye lubricants moisten eyes to alleviate discomfort such as the burning and irritation associated with xerophthalmia. They are also used to moisten contact lenses and artificial eyes. During anesthesia and in acute or chronic central nervous system (CNS) disorders that result in unconsciousness or decreased blinking, lubricants keep eyes moist and maintain the integrity of the epithelial surface of the eye.
Many brands and forms of ocular lubricants (artificial tears) are available OTC without a prescription. Although these agents are typically safe, the nurse must be alert to potential allergic reactions to preservatives found in lubricants.
Glaucoma and Ocular Hypertension Drugs
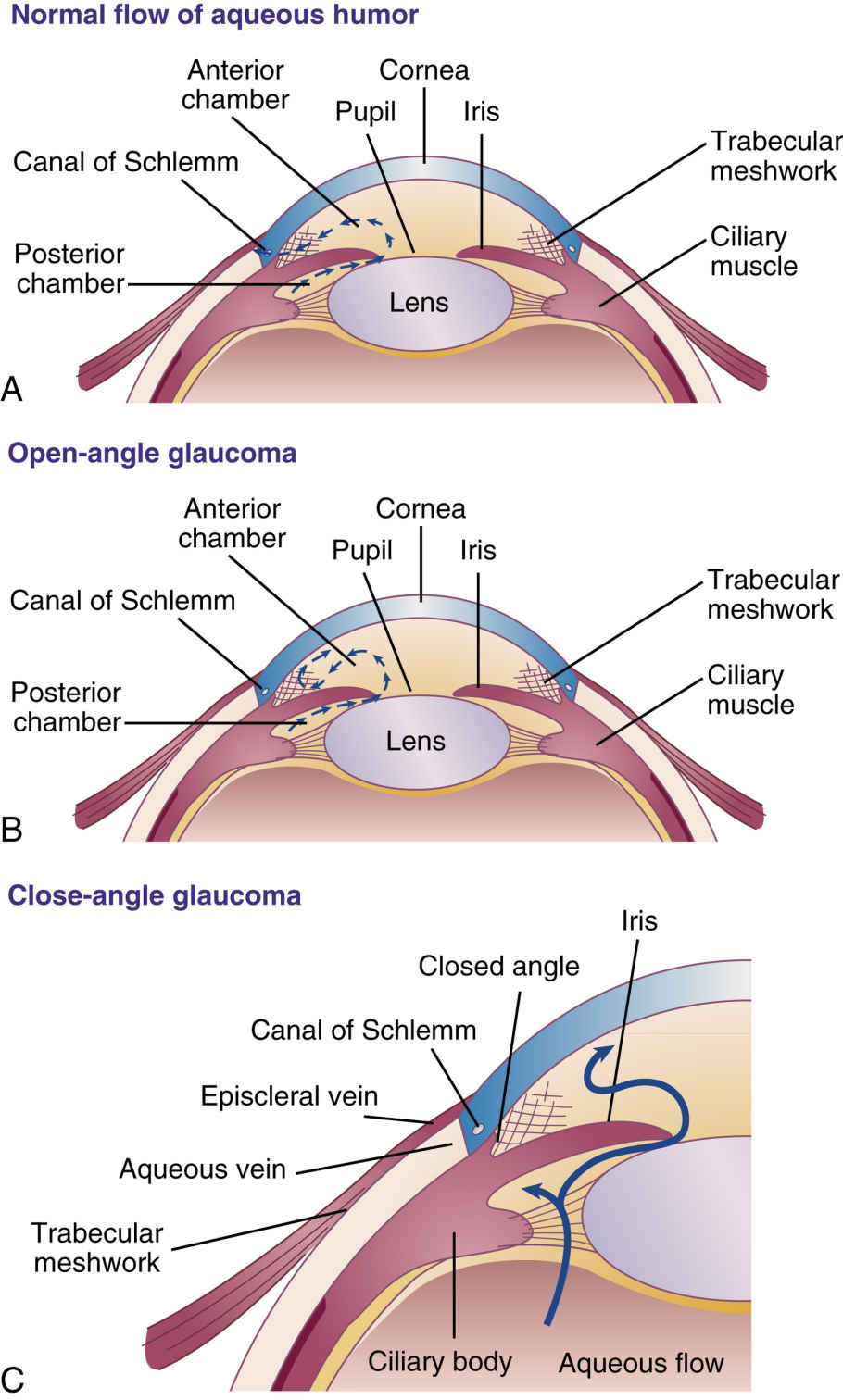
In the anterior chamber of the eye, aqueous humor, a clear fluid, flows continuously in and out of the chamber. As aqueous humor is formed, excess fluid drains through the trabecular meshwork structure of the eye and out the canal of Schlemm, with a much smaller fraction of the fluid exiting through the uveoscleral structure at the root of the iris (Fig. 44.1A). Overproduction of the fluid or improper drainage causes IOP to increase, and this buildup of pressure can damage the optic nerve and result in glaucoma. Without treatment, permanent vision loss can occur.
There are two types of glaucoma, open-angle and angle-closure. In open-angle glaucoma, the trabecular network is open but becomes clogged (see Fig. 44.1B). Over time, as blockage of the trabecular network worsens, the IOP gradually increases, which damages the optic nerve.
In angle-closure glaucoma, also known as closed-angle or narrow-angle glaucoma, the iris is situated close to the drainage angle blocking the trabecular network (see Fig. 44.1C). Because the excess aqueous humor cannot drain, it builds up within the eye and increases IOP. When the drainage angle is completely blocked, eye pressure increases quickly, and the vision becomes suddenly blurred; this is a medical emergency and must be treated immediately. Management of angle-closure glaucoma is often surgical; however, pharmacologic management is sometimes indicated.  Anticholinergic drugs (see Chapter 16) can cause mydriasis and can worsen angle-closure glaucoma.
Anticholinergic drugs (see Chapter 16) can cause mydriasis and can worsen angle-closure glaucoma.
Anticholinergic drugs (see Chapter 16) can cause mydriasis and can worsen angle-closure glaucoma.Glaucoma is further classified as either primary or secondary. Primary glaucoma occurs because of a pathologic change within the eye that happens without a known cause. Primary open-angle glaucoma (POAG), the most common type of glaucoma, is a chronic condition that develops slowly over time as the trabecular meshwork becomes clogged for unknown reasons. Secondary glaucoma occurs in response to a known cause such as injury, disease, or medication. Although a number of drugs can increase the risk of secondary glaucoma, those that cause pupillary dilation are particularly problematic because they give the iris more flexibility to move toward the drainage angle, blocking the trabecular meshwork. People who are at risk for glaucoma should avoid decongestants. Certain herbal preparations (e.g., goldenseal, ephedra, and bitter orange) can also create problems when given to patients who have glaucoma.
 Patient Safety
Patient SafetyHerbs that should be avoided in patients with glaucoma include bitter orange, blood root, celandine, coffee, corkwood, ephedra, goldenseal, and jimsonweed. Because all herbs have inherent risks, it is important to receive approval from the patient’s health care provider before recommending herbal preparations.
Drugs for glaucoma (Table 44.4) belong to one of six drug categories: (1) prostaglandin analogues, (2) beta-adrenergic blockers, (3) alpha-adrenergic agonists, (4) cholinergic agents, (5) carbonic anhydrase inhibitors, or (6) systemic hyperosmotic drugs. Prostaglandin analogues and beta-adrenergic blockers are typically first-line therapy, followed by alpha-adrenergic agonists. Each category acts in different ways to decrease IOP. Even though damage due to glaucoma cannot be reversed, treatments may prevent further damage.



Prostaglandin Analogues
Prostaglandin analogues are first-line drugs used primarily in the treatment of open-angle glaucoma and ocular hypertension. These drugs decrease IOP by improving trabecular outflow and by increasing the uveoscleral pathway, which is an alternate pathway of aqueous humor outflow. Examples of prostaglandin analogues include bimatoprost, latanoprost (Prototype Drug Chart 44.1), tafluprost, and travoprost. Prostaglandin analogues are taken at bedtime.
Side Effects and Adverse Reactions
Prostaglandin analogues used for glaucoma have unique side effects. These drugs gradually change the color of the iris by increasing brown pigmentation. This effect is most noticeable in individuals with green-brown and yellow-brown irises, and may be permanent. Darkening of the eyelids may also occur. Another side effect is the development of eyelash hypertrichosis, which is a growth in the number, length, thickness, and pigmentation of eyelashes. Patients may also develop macular edema, blurred vision, redness of the conjunctiva, and itching or stinging of the eye. Systemic effects such as bronchospasm, dizziness, dyspnea, and myalgia are rare. Prostaglandin analogues are generally better tolerated than alternative drugs for glaucoma.
Cholinergic Agents
Ophthalmic cholinergic agents cause miosis, a constriction of the pupil and contraction of the ciliary muscle. These actions result in a widening of the trabecular meshwork to improve outflow of excess aqueous humor. Additionally, as the pupil constricts, it straightens the iris, thus opening or widening the drainage angle to relieve angle-closure glaucoma. The two types of cholinergics are cholinergic agonists and cholinesterase inhibitors. Although their outcomes are similar, cholinergic agonists and cholinesterase inhibitors differ in their mechanism of action.
Cholinergic agonists are direct-acting cholinergics that directly stimulate cholinergic receptors. As a result, these drugs have the same action as the parasympathetic neurotransmitter acetylcholine. Pilocarpine is an example of a cholinergic agonist.
Cholinesterase inhibitors such as echothiophate are indirect-acting cholinergics, which inactivate the enzyme cholinesterase that typically breaks down acetylcholine. By inhibiting enzymatic destruction of acetylcholine, more acetylcholine is available to stimulate cholinergic receptors in the eye.
Side Effects and Adverse Reactions
Systemic absorption of cholinesterase inhibitors through the conjunctiva and lacrimal duct can produce systemic parasympathomimetic effects that include cardiac irregularities, diarrhea, hyperhidrosis, respiratory depression, and urinary incontinence. Other adverse effects from cholinesterase inhibitors include iritis, uveitis, and retinal detachment in addition to common complaints such as ocular irritation and pain, lacrimation, myopia with blurred vision, and paradoxical ocular hypertension. Systemic effects from cholinergic agonists are rare; ocular adverse effects are similar to those of the cholinesterase inhibitors. Cholinergic agonists and cholinesterase inhibitors are contraindicated for use in persons with closed-angle glaucoma.
Figs. 44.1B and C illustrate increased IOP resulting in open-angle and angle-closure glaucoma. Refer to Chapter 16 for more information on cholinergic drugs.
Beta-Adrenergic Blockers
Selective and nonselective beta-adrenergic blockers and beta blockers are first-line drugs used in the treatment of glaucoma. Beta-adrenergic blockers decrease IOP by decreasing the production of aqueous humor. Examples of ophthalmic nonselective beta-adrenergic blockers include carteolol, levobunolol, and timolol (Prototype Drug Chart 44.2). Selective ocular beta blockers include betaxolol.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


