• Secondary EMPD has more variable immunohistochemical profile
Secondary EMPD associated with urothelial carcinoma is CK7 and CK20(+)
Secondary EMPD associated with anal/rectal carcinoma is CK20(+) and CK7(-)
Top Differential Diagnoses
• Squamous cell carcinoma in situ
• Melanoma in situ
• Clear cell papulosis
• Benign mucinous metaplasia of penis
• Pagetoid dyskeratosis
• Pagetoid reticulosis
• Melanoma in situ
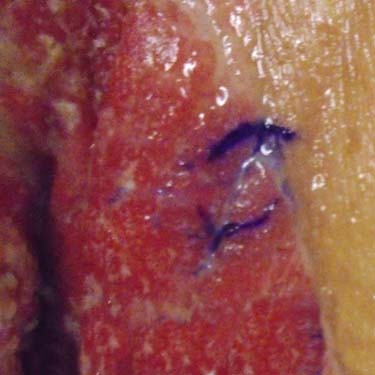
Clinical Appearance of EMPD This case presented as a large, moist-appearing erythematous patch affecting the groin of an elderly patient.
Paget Cells Involving All Levels of Epidermis Large, pale-staining neoplastic cells extensively infiltrate all levels of the hyperplastic epidermis in another case of extramammary Paget disease (EMPD). There is a chronic inflammatory infiltrate in the upper dermis.
Hyperplastic Epidermis With Marked Pagetoid Spread in EMPD The epidermis in this case shows hyperplasia with papillary features. The neoplastic cells are numerous and affect all levels of the epidermis, including the stratum corneum . They are arranged as single units and confluent aggregates.
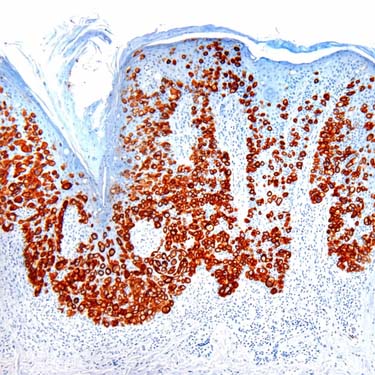
CK7 Expression in EMPD CK7 immunohistochemical stain strongly highlights the neoplastic cells throughout the epidermis. The use of CK7 may also assist in defining the margins of the disease.
TERMINOLOGY
Abbreviations
• Extramammary Paget disease (EMPD)
Definitions
• Adenocarcinoma involving epidermis and commonly extending to epithelium of eccrine glands &/or hair follicles (adenocarcinoma in situ)
• May involve dermis in minority of cases
ETIOLOGY/PATHOGENESIS
Pathogenesis
• Uncertain in most cases
• Cases limited to epidermis are postulated to originate from intraepidermal portion of sweat glands or from intraepidermal stem cells
• Heterogeneous condition; can be classified as primary (cutaneous origin) and secondary (extracutaneous origin)
Primary EMPD is rarely associated with underlying sweat gland carcinoma (usually apocrine)
Secondary EMPD: Associated with internal carcinoma in 15-29% of cases
– Genital EMPD is often associated with genitourinary carcinomas and perianal EMPD is more frequently associated with gastrointestinal carcinomas
– Most frequent in perianal EMPD (underlying rectal carcinoma in 1/3 of cases)
CLINICAL ISSUES
Epidemiology
• Age
6th-8th decades
• Sex
F > M
Site
• Skin regions rich in apocrine glands
Most common sites: Vulva and perianal region
Other sites: Scrotum, perineum, penis, axilla, umbilicus
Exceptional sites: Eyelid (accompanying carcinoma of Moll gland), external auditory meatus (associated with ceruminous carcinoma), face, scalp, chest, abdomen, and extremities
Presentation
• Circinate or annular moist erythematous scaly patches or plaques
• Other presentations: Gray-white eczematous patches, hypopigmented or pigmented macules, ulcerated plaques/tumors
• Pruritus is frequent and may precede clinical lesion
• Bleeding, oozing, tenderness, or burning sensation can occur
• EMPD may mimic eczema
• Lesions may be multifocal
Treatment
• Complete surgical excision is treatment of choice for primary EMPD
Patients require long-term follow-up because of multifocal nature of condition and high recurrence rate
• Treatment in secondary lesions will depend on associated carcinoma
Only gold members can continue reading. Log In or Register to continue



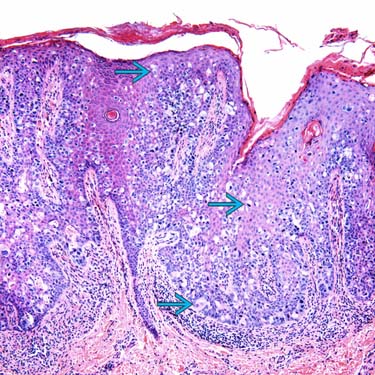
 extensively infiltrate all levels of the hyperplastic epidermis in another case of extramammary Paget disease (EMPD). There is a chronic inflammatory infiltrate in the upper dermis.
extensively infiltrate all levels of the hyperplastic epidermis in another case of extramammary Paget disease (EMPD). There is a chronic inflammatory infiltrate in the upper dermis.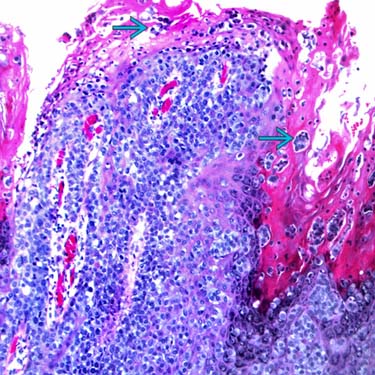
 . They are arranged as single units and confluent aggregates.
. They are arranged as single units and confluent aggregates.