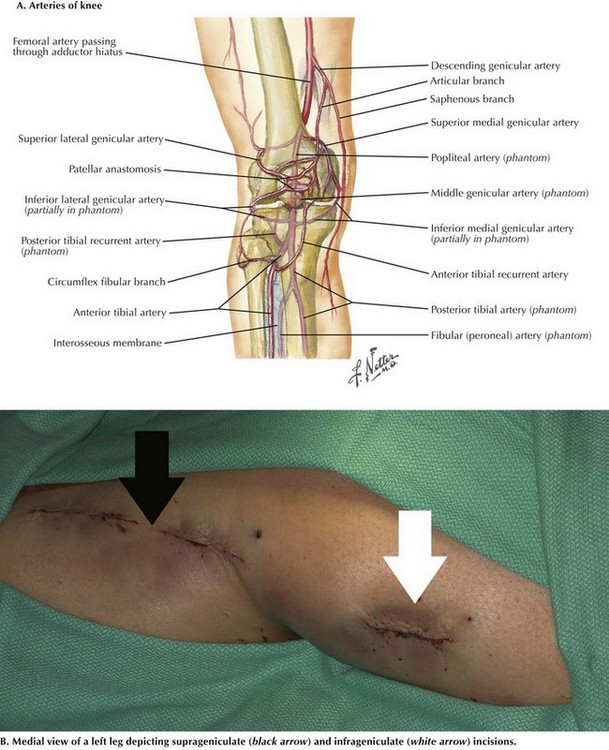
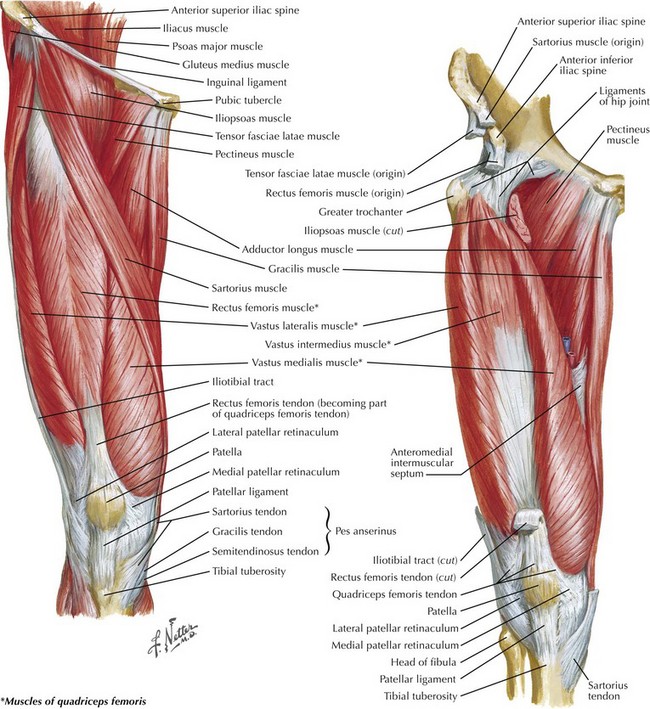
Chapter 38 The popliteal artery begins at the adductor canal within the adductor magnus muscle (Hunter’s canal) as it enters the popliteal space behind the knee joint. The popliteal artery ends when it splits in the lower leg to become the anterior tibial artery and tibioperoneal trunk. Several important geniculate collaterals increase in caliber in cases of progressive atherosclerotic occlusion of the distal superficial femoral and popliteal arteries (Fig. 38-1, A). If an acute occlusion is present in this area, however, the collateral vessels are not sufficient and the leg is usually threatened, requiring immediate revascularization. Venous anatomy, on the other hand, is more variable. The medial suprageniculate approach is most often used in femoral-to-popliteal artery (femoropopliteal) bypass above the knee. The patient is placed in the supine position with the knee slightly flexed. An incision is made on the distal portion of the medial thigh over the estimated location of the sartorius muscle (Fig. 38-1, B). After locating the junction between the sartorius (posterior) and vastus medialis (anterior), the surgeon places a self-retaining retractor there (Fig. 38-2).
Exposure of the Popliteal Artery and Vein

Surgical Principles
Medial Suprageniculate Approach
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine