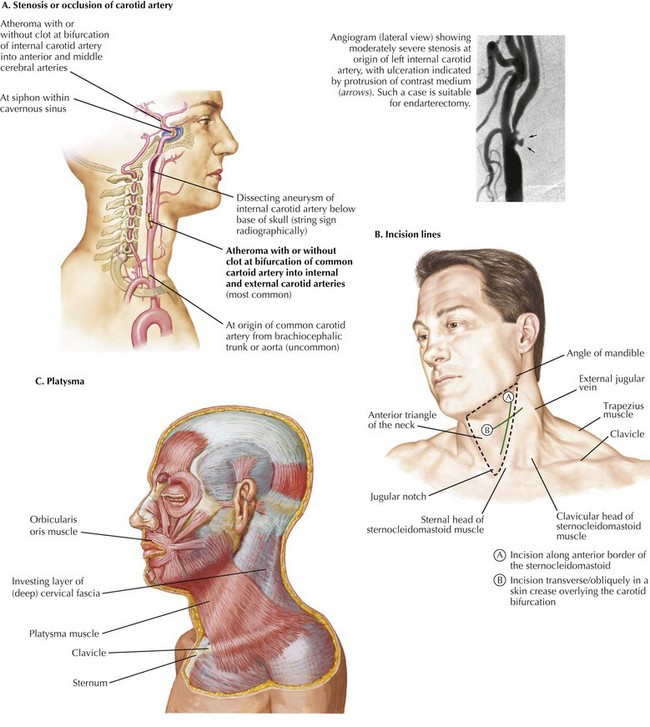
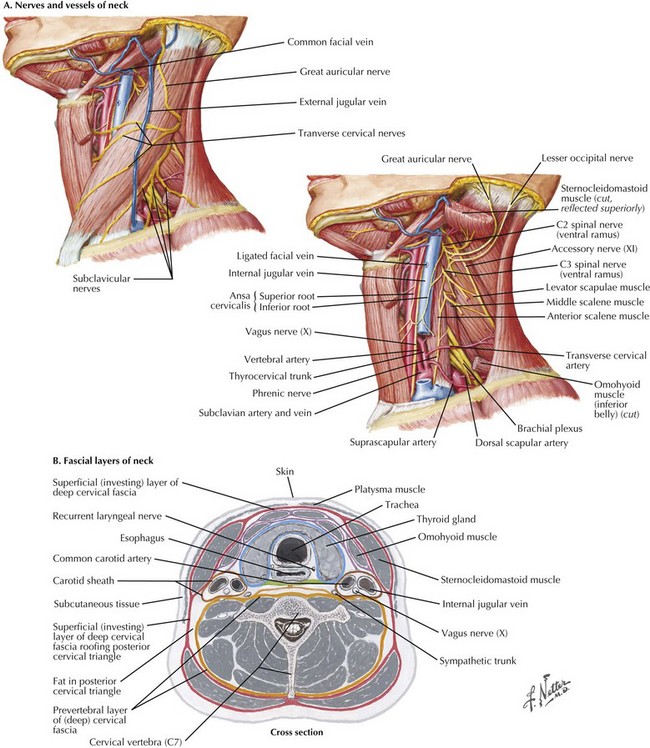
Chapter 32 Carotid endarterectomy is one of the most frequently performed vascular operations. The vast majority of these procedures are for atherosclerosis at the bifurcation of the common carotid artery, which lies within the anterior triangle of the neck, usually at the upper border of the thyroid cartilage (Fig. 32-1, A). The key anatomic boundaries are the sternocleidomastoid muscle, the midline, and the mandible (Fig. 32-1, B). The procedure begins with proper positioning of the patient, with the neck extended and turned toward the opposite side. The incision can be made along the anterior border of the sternocleidomastoid muscle (SCM) or transversely (obliquely) in a skin crease overlying the carotid bifurcation (Fig. 32-1, B). The bifurcation can easily be located with duplex ultrasound. The platysma muscle is then divided, exposing the deep cervical fascia (Fig. 32-1, C). The external jugular vein and greater auricular nerve lie in this plane; the vein can be ligated, but the nerve must be preserved to avoid numbness of the ear lobe (Fig. 32-2, A). Next, two key steps are necessary to expose the carotid bifurcation. The first is mobilization of the anterior border of the SCM, which is invested within two layers of the deep cervical fascia (Fig. 32-2, B). If a transversely oriented incision is used, this requires creation of subplatysmal flaps, both cephalad and caudad, on the plane of the anterior SCM fascial layer. The ansa cervicalis nerve (also known as ansa hypoglossi) is often seen running along the anterior surface of the common carotid artery (Fig. 32-2, A). This nerve can be divided with impunity, and the cranial end followed to its junction with the hypoglossal nerve. The hypoglossal nerve runs between the internal jugular vein and internal carotid artery and is usually found about 2 cm above the carotid bifurcation. However, its position can vary. Often, small jugular venous tributaries drain the SCM at this level, along with accompanying arteries that must be divided. Extreme care must be taken to avoid bleeding in this location; attempts to control bleeding are a common cause of injury to the hypoglossal nerve.
Exposure of the Carotid Bifurcation

Introduction
Carotid Endarterectomy
Surgical Principles
Anatomic Landmarks
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine