EBV+ Diffuse Large B-cell Lymphoma of the Elderly
Tarlq Muzzzafar, MBBS
Key Facts
Terminology
DLBCL infected by EBV occurring in patients > 50 years old without history of immunodeficiency or lymphoma
Clinical Issues
Median age: ˜ 70 years (range: 45-92 years)
Affected patients are relatively healthy prior to diagnosis
Extranodal mass ± lymphadenopathy in ˜ 70%
Only lymphadenopathy in ˜ 30%
Median survival is 2 years
Microscopic Pathology
EBV(+) DLBCL-E effaces architecture of extranodal site &/or lymph node
2 subtypes: Polymorphous and large cell lymphoma (monomorphous)
Represent a morphologic spectrum
No clinical or prognostic relevance
Sheets of necrosis; often with geographic pattern
Ancillary Tests
CD20(+), CD22(+), CD79α(+), pax-5(+)
IRF-4/MUM1(+), CD30(+/-)
Ki-67 (MIB1) shows high proliferation index
Lymphoma cells have EBV type III latency pattern
EBV present in monoclonal episomal form
Top Differential Diagnoses
DLBCL, not otherwise specified
Plasmablastic lymphoma
Classical Hodgkin lymphoma
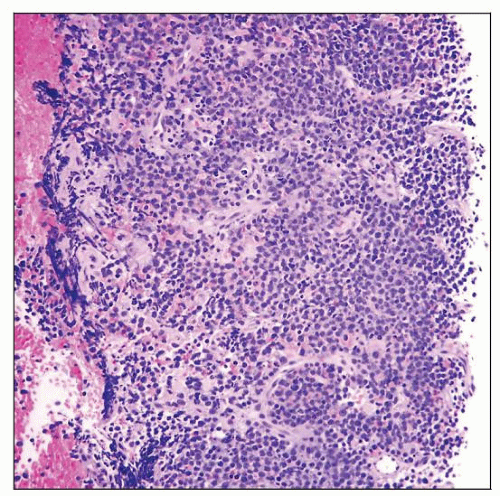 EBV(+) diffuse large B-cell lymphoma of the elderly (EBV[+] DLBCL-E) involving needle biopsy of thigh mass. This neoplasm is the monomorphous subtype and is composed of sheets of lymphoma cells. |
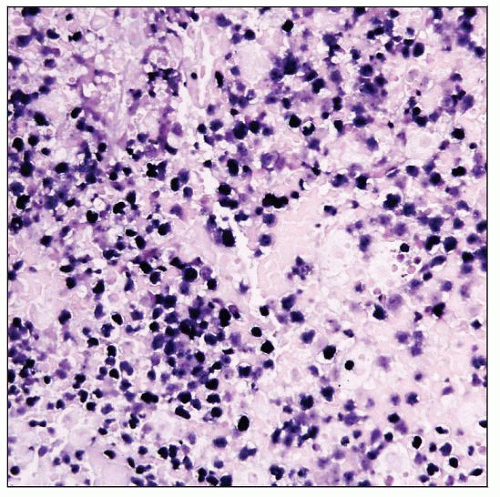 EBV(+) DLBCL-E, monomorphous subtype involving needle biopsy of thigh mass. In situ hybridization analysis shows that the lymphoma cells are strongly positive for EBV small encoded RNA (EBER). |
TERMINOLOGY
Abbreviations
Epstein-Barr virus(EBV) diffuse large B-cell lymphoma of the elderly (DLBCL-E)
Synonyms
Senile EBV(+) B-cell lymphoproliferative disorder
Age-related EBV(+) lymphoproliferative disorder
EBV-associated B-cell lymphoproliferative disorder of the elderly
Definitions
DLBCL infected by EBV occurring in patients > 50 years old without history of immunodeficiency or lymphoma
These tumors exhibit a broad morphologic spectrum from polymorphous and Hodgkin-like lesions to monotonous DLBCL
ETIOLOGY/PATHOGENESIS
Epstein-Barr Virus (EBV) Drives B-cell Transformation and Lymphoproliferation
EBV: γ-herpes virus ubiquitous in humans
> 90% of humans are infected
Most have lifelong asymptomatic infection
EBV can infect B, T, and NK cells as well as epithelial cells
Increased risk for EBV-associated lymphomas in patients with
Congenital immunodeficiency
Acquired immunodeficiency
Human immunodeficiency virus infection
Iatrogenic causes
Elderly adults in apparent good health recently identified as at-risk group
Impaired immunity associated with aging is implicated
In particular, impaired host T-cell surveillance
When EBV infects B cells, the virus will
Upregulate and activate multiple cell signaling pathways and antiapoptotic proteins
Induce B-cell proliferation and transformation
In EBV(+) DLBCL-E, virus shows type III EBV latency pattern
All EBV nuclear antigens (EBNAs), EBER, and latent membrane proteins (LMPs) are expressed
CLINICAL ISSUES
Epidemiology
Incidence
In Asian countries, EBV(+) DLBCL-E represents up to 10% of all DLBCL cases in patients without apparent immunodeficiency
Apparently less common in Western nations; little data available
Age
Median: ˜ 70 years (range: 45-92 years)
˜ 25% of patients ≥ 90 years
Gender
M:F = 1.4:1
Site
Extranodal sites involved in 70% of patients
Skin, lung, tonsil, and stomach most common
Bone marrow or blood involved in ˜ 10% of patients
Lymph nodes
Presentation
Affected patients are relatively healthy prior to diagnosis
Extranodal mass ± lymphadenopathy in ˜ 70% of patients
Only lymphadenopathy in ˜ 30% of patients
B symptoms in ˜ 60% of patients
High International Prognostic Index (IPI) score in ˜ 60% of patients
Ann Arbor stage III-IV in ˜ 60% of patients
Laboratory Tests
˜ 50% of patients have elevated lactate dehydrogenase (LDH) level
Treatment
Drugs
Consensus for specific chemotherapy regimen has not been established
Cyclophosphamide, adriamycin, vincristine, and prednisone (CHOP) regimen has been used
Clinical remission achieved in 63%
Response worse than in patients with EBV(-) DLBCL
Role of rituximab has not been determined
Prognosis
Median survival is 2 years
Presence of B symptoms and age > 70 years indicate worse prognosis
MICROSCOPIC PATHOLOGY
Histologic Features
EBV(+) DLBCL-E effaces architecture of extranodal site &/or lymph node
2 subtypes: Polymorphous and large cell lymphoma (monomorphous)
Represent a morphologic spectrum
Distinguishing these subtypes histologically can be arbitrary in some cases
No clinical or prognostic relevance
Both types demonstrate
Large lymphoma cells and Hodgkin and Reed-Sternberg (HRS)-like cells
Increased mitotic activity
Sheets of necrosis; often with geographic pattern
Polymorphous subtype
Broad spectrum of B-cell maturation
Polymorphous reactive infiltrate in background: Small lymphocytes, plasma cells, and histiocytes
Monomorphous subtype
Sheets of large monomorphous cells resembling DLBCL
Cytologic Features
Large lymphoma cells can be centroblastic, immunoblastic, or plasmablastic
ANCILLARY TESTS
Immunohistochemistry
CD20(+), CD22(+), CD79a(+), pax-5(+)
IRF4/MUM1(+), CD30(+/-)
± monotypic cytoplasmic immunoglobulin light chain in cells with plasmacytoid differentiation
Ki-67 (MIB1) shows high proliferation index
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


