Patient Story
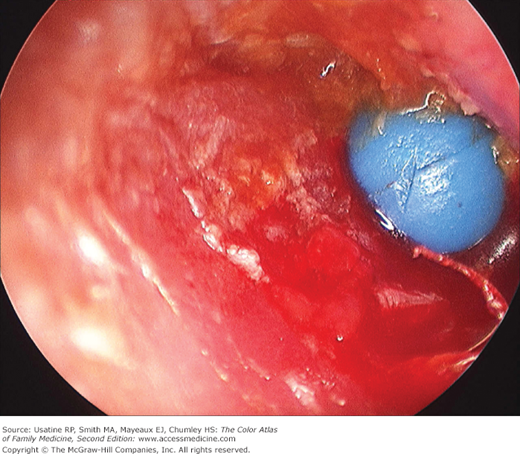
A 3-year-old girl is brought by her parents to an urgent care facility after a day of crying, irritability, scant otorrhea, and frequent pulling of her right ear. Otoscopy reveals an erythematous, swollen external auditory canal (EAC) where a bead is wedged (Figure 28-1). The patient is referred to an otolaryngologist and the bead is removed using an operating microscope for visualization.
Introduction
Epidemiology
Etiology and Pathophysiology
- Most common FBs in children include:5
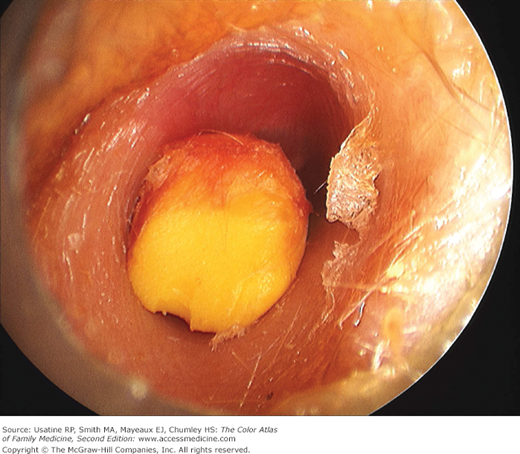
- Inanimate objects such as beads (see Figure 28-1), cotton tips, paper, toy parts, crayons (Figure 28-2), eraser tips, food, or organic matter, including sand (Figure 28-3), sticks, and stones.
- Insects (Figure 28-4).
- Inanimate objects such as beads (see Figure 28-1), cotton tips, paper, toy parts, crayons (Figure 28-2), eraser tips, food, or organic matter, including sand (Figure 28-3), sticks, and stones.
- Pathogenesis includes some of the key elements of otitis externa (see Chapter 27, Otitis Externa):
- Initial breakdown of the skin-cerumen barrier (caused by presence of FB).
- Skin inflammation and edema leading to subsequent obstruction of adnexal structures (e.g., cerumen glands, sebaceous glands, and hair follicles).
- FB reaction leading to further skin injury.
- In the case of alkaline battery electrochemical reaction, severe alkaline burns may occur.
- Initial breakdown of the skin-cerumen barrier (caused by presence of FB).


Risk Factors
- Children with attention deficit hyperactivity disorder (ADHD) may be more likely to self-insert FBs and ADHD should be considered in children with ear FBs who are older than age 5 years.6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


