High-Yield Terms to Learn
Angina of effort, classic angina, atherosclerotic angina Angina pectoris (crushing, strangling chest pain) that is precipitated by exertion, that is, increased O2 demand that cannot be met because of relatively irreversible atherosclerotic obstruction of coronary arteries
Vasospastic angina, variant angina, Prinzmetal’s angina Angina precipitated by reversible spasm of coronary vessels Coronary vasodilator Older, incorrect name for drugs useful in angina; drugs that relieve angina of effort do not usually act primarily through coronary vasodilation; some potent coronary vasodilators are ineffective in angina “Monday disease” Industrial disease caused by chronic exposure to vasodilating concentrations of organic nitrates in the workplace; characterized by headache, dizziness, and tachycardia on return to work after 2 days absence Nitrate tolerance, tachyphylaxis Loss of effect of a nitrate vasodilator when exposure is prolonged beyond 10-12 h Unstable angina Rapidly progressing increase in frequency and severity of anginal attacks, especially pain at rest; an acute coronary syndrome and often heralds imminent myocardial infarction Preload Filling pressure of the heart, dependent on venous tone and blood volume; determines end-diastolic fiber length and tension Afterload Resistance to ejection of stroke volume; determined by arterial blood pressure and arterial stiffness; afterload determines systolic fiber tension Intramyocardial fiber tension Force exerted by myocardial fibers, especially ventricular fibers at any given time; a primary determinant of O2 requirement
Double product The product of heart rate and systolic blood pressure; an estimate of cardiac work Myocardial revascularization Mechanical intervention to improve O2 delivery to the myocardium by angioplasty or bypass grafting
Pathophysiology of Angina
Types of Angina
Atherosclerotic Angina
Atherosclerotic angina is also known as angina of effort or classic angina. It is associated with atheromatous plaques that partially occlude 1 or more coronary arteries. When cardiac work increases (eg, in exercise), the obstruction of flow and inadequate oxygen delivery results in the accumulation of acidic metabolites and ischemic changes that stimulate myocardial pain endings. Rest usually leads to complete relief of the pain within 15 min. Atherosclerotic angina constitutes about 90% of angina cases.
Vasospastic Angina
Vasospastic angina, also known as rest angina, variant angina, or Prinzmetal’s angina, is responsible for less than 10% of cases. It involves reversible spasm of coronaries, usually at the site of an atherosclerotic plaque. Spasm may occur at any time, even during sleep. Vasospastic angina may deteriorate into unstable angina.
Unstable Angina
A third type of angina—unstable or crescendo angina, also known as acute coronary syndrome —is characterized by increased frequency and severity of attacks that result from a combination of atherosclerotic plaques, platelet aggregation at fractured plaques, and vasospasm. Unstable angina is thought to be the immediate precursor of a myocardial infarction and is treated as a medical emergency.
Determinants of Cardiac Oxygen Requirement
The pharmacologic treatment of coronary insufficiency is based on the physiologic factors that control myocardial oxygen requirement. A major determinant is myocardial fiber tension (the higher the tension, the greater the oxygen requirement).
Several variables contribute to fiber tension (Figure 12-1), as discussed next.
FIGURE 12-1
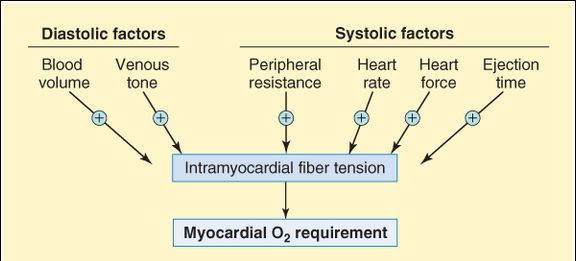
Determinants of the volume of oxygen required by the heart. Both diastolic and systolic factors contribute to the oxygen requirement; most of these factors are directly influenced by sympathetic discharge (venous tone, peripheral resistance, heart rate, and heart force).
Preload and Afterload
Preload (diastolic filling pressure) is a function of blood volume and venous tone. Venous tone is mainly controlled by sympathetic outflow. Afterload is determined by arterial blood pressure and large artery stiffness. It is one of the systolic determinants of oxygen requirement.
Heart Rate
Heart rate contributes to total fiber tension because at fast heart rates, fibers spend more time at systolic tension levels. Furthermore, at faster rates, diastole is abbreviated, and diastole constitutes the time available for coronary flow (coronary blood flow is low or nil during systole).
Heart rate and systolic blood pressure may be multiplied to yield the double product, a measure of cardiac work and therefore of oxygen requirement. As intensity of exercise (eg, running on a treadmill) increases, demand for cardiac output increases, so the double product also increases. However, the double product is sensitive to sympathetic tone, as is cardiac oxygen demand (Figure 12-1). In patients with atherosclerotic angina, effective drugs reduce the double product by reducing cardiac work without reducing exercise capacity.
Cardiac Contractility
Force of cardiac contraction is another systolic factor controlled mainly by sympathetic outflow to the heart. Ejection time for ventricular contraction is inversely related to force of contraction but is also influenced by impedance to outflow. Increased ejection time (prolonged systole) increases oxygen requirement.
Therapeutic Strategies
The defect that causes anginal pain is inadequate coronary oxygen delivery relative to the myocardial oxygen requirement. This defect can be corrected—at present—in 2 ways: by increasing oxygen delivery and by reducing oxygen requirement (Figure 12-2). Traditional pharmacologic therapies include the nitrates, the calcium channel blockers, and the  blockers.
blockers.
FIGURE 12-2
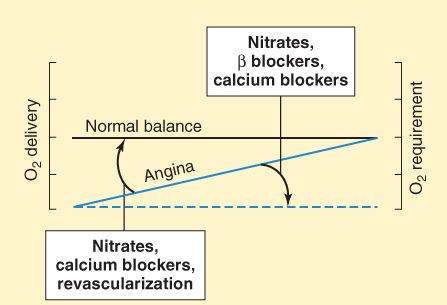
Strategies for the treatment of angina pectoris. When coronary flow is adequate, O2 delivery is equal to O2 requirement (horizontal black line). Angina is characterized by reduced coronary oxygen delivery versus oxygen requirement (oblique solid blue line). In some cases, this can be corrected by increasing oxygen delivery (box on left: revascularization or, in the case of reversible vasospasm, nitrates and calcium channel blockers). More often, drugs are used to reduce oxygen requirement (box on right: nitrates,  blockers, and calcium channel blockers) and cause a shift to the dashed blue line.
blockers, and calcium channel blockers) and cause a shift to the dashed blue line.
A newer strategy attempts to increase the efficiency of oxygen utilization by shifting the energy substrate preference of the heart from fatty acids to glucose. Drugs that may act by this mechanism are termed partial fatty acid oxidation inhibitors (pFOX inhibitors) and include ranolazine and trimetazidine. However, more recent evidence suggests that the major mechanism of action of ranolazine is inhibition of late sodium current (see below). Another new group of antianginal drugs selectively reduces heart rate with no other detectable hemodynamic effects. These investigational drugs (ivabradine is the prototype) act by inhibition of the sinoatrial pacemaker current, If.
The nitrates, calcium blockers, and  blockers all reduce the oxygen requirement in atherosclerotic angina. Nitrates and calcium channel blockers (but not
blockers all reduce the oxygen requirement in atherosclerotic angina. Nitrates and calcium channel blockers (but not  blockers) can also increase oxygen delivery by reducing spasm in vasospastic angina. Myocardial revascularization corrects coronary obstruction either by bypass grafting or by angioplasty (enlargement of the lumen by means of a special catheter). Therapy of unstable angina differs from that of stable angina in that urgent angioplasty is the treatment of choice in most patients and platelet clotting is the major target of drug therapy. The platelet glycoprotein IIb/IIIa inhibitors—abciximab, eptifibatide, and tirofiban—are used in this condition (see Chapter 34). Intravenous nitroglycerin is sometimes of value.
blockers) can also increase oxygen delivery by reducing spasm in vasospastic angina. Myocardial revascularization corrects coronary obstruction either by bypass grafting or by angioplasty (enlargement of the lumen by means of a special catheter). Therapy of unstable angina differs from that of stable angina in that urgent angioplasty is the treatment of choice in most patients and platelet clotting is the major target of drug therapy. The platelet glycoprotein IIb/IIIa inhibitors—abciximab, eptifibatide, and tirofiban—are used in this condition (see Chapter 34). Intravenous nitroglycerin is sometimes of value.
Nitrates
Classification and Pharmacokinetics
Nitroglycerin (the active ingredient in dynamite) is the most important of the therapeutic nitrates and is available in forms that provide a range of durations of action from 10-20 min (sublingual) to 8-10 h (transdermal) (see the Drug Summary Table at the end of the chapter). Because treatment of acute attacks and prevention of attacks are both important aspects of therapy, the pharmacokinetics of these different dosage forms are clinically significant.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


