Drugs Used in Acid-Peptic Disease
Ulceration and erosion of the lining of the upper portion of the gastrointestinal tract are common problems that manifest as gastroesophageal reflux disease (GERD), gastric and duodenal peptic ulcers, and stress-related mucosal injury. Drugs used in acid-peptic disease reduce intragastric acidity by manipulating systems controlling hydrogen acid secretion (Figure 59-1), promote mucosal defense or, in the case of peptic ulcers, eradicate the bacterium Helicobacter pylori, which is detectable in over 80% of patients with duodenal ulcers.
FIGURE 59-1
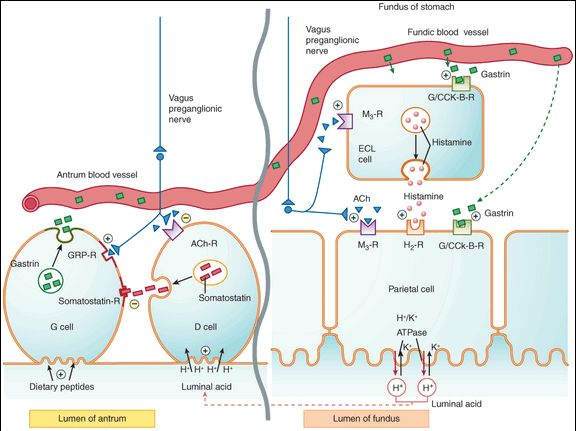
Schematic model of physiologic control of hydrogen ion (acid) secretion by the gastric parietal cells, which are stimulated by gastrin (acting on gastrin/CCK-B receptors), acetylcholine (ACh; M3 receptor), and histamine (H2 receptor). Acid is secreted across the parietal cell canalicular membrane by the H+/K+ ATPase proton pump into the gastric lumen. The gastrin that is secreted by antral G cells in response to intraluminal dietary peptides acts directly on parietal cells and also stimulates release of histamine from enterochromaffin-like (ECL) cells. The vagus nerve stimulates postganglionic neurons of the enteric nervous system to release acetylcholine ACh, which acts on parietal and ECL cells. In the antrum, release of gastrin-releasing peptide (GRP) from postganglionic neurons directly increases gastrin release, whereas release of ACh indirectly increases gastrin secretion by inhibiting release of somatostatin from antral D cells. The increase in intraluminal H+ concentration causes D cells to release somatostatin and thereby inhibit gastrin release from G cells. CCK, cholecystokinin; R, receptor.
(Reproduced, with permission, from Katzung BG, editor: Basic & Clinical Pharmacology, 11th ed. McGraw-Hill, 2009: Fig. 62-1.)
Antacids
Antacids are weak bases that neutralize stomach acid by reacting with protons in the lumen of the gut and may also stimulate the protective functions of the gastric mucosa. When used regularly in the large doses needed to significantly raise the stomach pH, antacids reduce the recurrence rate of peptic ulcers.
The antacids differ mainly in their absorption and effects on stool consistency. Popular antacids include magnesium hydroxide (Mg[OH]2) and aluminum hydroxide (Al[OH]3). Neither of these weak bases is significantly absorbed from the bowel. Magnesium hydroxide has a strong laxative effect, whereas aluminum hydroxide has a constipating action. These drugs are available as single-ingredient products and as combined preparations. Calcium carbonate and sodium bicarbonate are also weak bases, but they differ from aluminum and magnesium hydroxides in being absorbed from the gut. Because of their systemic effects, calcium and bicarbonate salts are less popular as antacids.
H2-Receptor Antagonists
Cimetidine and other H2 antagonists (ranitidine, famotidine, and nizatidine) inhibit stomach acid production. They are effective in the treatment of GERD, peptic ulcer disease, and nonulcer dyspepsia and in the prevention of stress-related gastritis in seriously ill patients. Although they are still used widely, their clinical use is being supplanted by the more effective and equally safe proton pump inhibitors. The H2 antagonists are described in detail in Chapter 16.
Proton Pump Inhibitors
Omeprazole and other proton pump inhibitors (esomeprazole, lansoprazole, pantoprazole, and rabeprazole) are lipophilic weak bases that diffuse into the parietal cell canaliculi, where they become protonated and concentrated more than 1000-fold. There they undergo conversion to compounds that irreversibly inactivate the parietal cell H+/K+ ATPase, the transporter that is primarily responsible for producing stomach acid. Oral formulations of these drugs are enteric coated to prevent acid inactivation in the stomach. After absorption in the intestine, they are rapidly metabolized in the liver, with half-lives of 1-2 h. However, their durations of action are approximately 24 h, and they may require 3-4 d of treatment to achieve their full effectiveness.
Proton pump inhibitors are more effective than H2 antagonists for GERD and peptic ulcer and equally effective in the treatment of nonulcer dyspepsia and the prevention of stress-related mucosal bleeding. They are also useful in the treatment of Zollinger-Ellison syndrome. Adverse effects of proton pump inhibitors occur infrequently and include diarrhea, abdominal pain, and headache. Chronic treatment with proton pump inhibitors may result in hypergastrinemia. However, there is no documentation that the use of these drugs increases the incidence of carcinoid or colon cancer. Proton pump inhibitors may decrease the oral bioavailability of vitamin B12 and certain drugs that require acidity for their gastrointestinal absorption (eg, digoxin, ketoconazole). Patients taking proton pump inhibitors may have a small increase in the risk of respiratory and enteric infections.
Sucralfate
An aluminum sucrose sulfate, sucralfate is a small, poorly soluble molecule that polymerizes in the acid environment of the stomach. The polymer binds to injured tissue and forms a protective coating over ulcer beds. Sucralfate accelerates the healing of peptic ulcers and reduces the recurrence rate. Unfortunately, sucralfate must be taken 4 times daily. Sucralfate is too insoluble to have significant systemic effects when taken by the oral route; toxicity is very low.
Misoprostol
An analog of PGE1 , misoprostol increases mucosal protection and inhibits acid secretion. It is effective in reducing the risk of ulcers in users of nonsteroidal anti-inflammatory drugs (NSAIDs) but is not widely used because of the need for multiple daily dosing and poorly tolerated adverse effects (gastrointestinal upset and diarrhea). Misoprostol is discussed in detail in Chapter 18.
Colloidal Bismuth
Bismuth has multiple actions, including formation of a protective coating on ulcerated tissue, stimulation of mucosal protective mechanisms, direct antimicrobial effects, and sequestration of enterotoxins. Bismuth subsalicylate, a nonprescription formulation of bismuth and salicylate, reduces stool frequency and liquidity in infectious diarrhea. Bismuth causes black stools.
Antibiotics
Chronic infection with H pylori is present in most patients with recurrent non-NSAID-induced peptic ulcers. Eradication of this organism greatly reduces the rate of recurrence of ulcer in these patients. One regimen of choice consists of a proton pump inhibitor plus a course of clarithromycin and amoxicillin (or metronidazole in patients with penicillin allergy).
Drugs That Promote Upper Gastrointestinal Motility
Prokinetic drugs that stimulate upper gastrointestinal motility are helpful for gastroparesis and for postsurgical gastric emptying delay. Their ability to increase lower esophageal sphincter pressures also makes them useful for some patients with GERD. In the past, cholinomimetic agonists such as bethanechol were used for GERD and gastroparesis, but the availability of less toxic agents has supplanted their use. The acetylcholinesterase inhibitor neostigmine is still used for the treatment of hospitalized patients with acute large bowel distention. The cholinomimetics are discussed in Chapter 7.
In the enteric nervous system, dopamine serves an inhibitory function by inhibiting cholinergic stimulation of smooth muscle contraction. Metoclopramide and domperidone are D2 dopamine receptor antagonists that promote gastrointestinal motility. The D2 receptor-blocking action of these drugs in the area postrema is also of value in preventing emesis after surgical anesthesia and emesis induced by cancer chemotherapeutic drugs. When used chronically, metoclopramide can cause symptoms of parkinsonism, other extrapyramidal effects, and hyperprolactinemia. Because it does not cross the blood-brain barrier, domperidone is less likely to cause CNS toxicity.
The antibiotic erythromycin (Chapter 44) promotes motility by stimulating motilin receptors. It may have benefit in some patients with gastroparesis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


