Disorders of the Lower Urinary Tract
Cheryl L. Brandt and Roberta J. Emerson
Key Questions
• How are congenital abnormalities of the urinary collecting system detected and treated?
• What are the risk factors and clinical manifestations for bladder cancer?
• How do stones in the lower urinary tract present clinically?

http://evolve.elsevier.com/Copstead/
The lower urinary tract encompasses several structures that together are responsible for the transport and elimination of urine from the body. These structures include the ureters, bladder, urethra, and associated urinary sphincters. The male prostate gland is anatomically located in this area, but is functionally involved in male reproduction; the role and disorders of the prostate gland are presented in Chapters 30 and 31, respectively.
Ureters collect the urine formed in the kidneys from the renal pelvises and transport it to the bladder. The bladder is a hollow, muscular reservoir for urine that expands to store it and then contracts to expel urine through the urethra. Urine storage depends on intact spinal reflexes. The process of micturition (voiding) involves both reflex and voluntary mechanisms, mediated by the micturation center in the pons. Voiding is a result of coordinated function of bladder mechanoreceptors, neurologic impulse transmission, bladder muscle contraction, and urethral sphincter relaxation.1
In addition to voiding dysfunction, disorders of the lower urinary tract can generally be classified as congenital, neoplastic, infective, inflammatory, or obstructive. These disorders are often interrelated. For instance, stasis of urine, which occurs with a variety of disorders, often leads to urinary tract infection (UTI). Infection of the kidney, pyelonephritis (see Chapter 27), and acute postrenal kidney injury (see Chapter 28) can be caused by any number of pathologies affecting the lower urinary tract. Lower urinary tract disorders can result in significant health problems that have tremendous physical, psychosocial, and economic ramifications on patients and their families.2–5
Lower Urinary Tract
The role of the lower urinary tract is to transport urine formed by the kidneys and allow its appropriate removal from the body. The anatomy of the lower urinary tract is presented in Chapter 26. Urine movement from the kidneys to the bladder is due to the effect of gravity facilitated by peristaltic movement of the ureters. The bladder stores the urine until it is released through the urethra, ultimately by conscious decision. Anatomic integrity of the ureters and bladder, competent urethral sphincters, and an appropriately functioning nervous system are required for the lower urinary system to properly carry out its role.
Diagnostic Tests
Several of the procedures presented in Chapter 26 are used to diagnose urologic disorders discussed in this chapter. Other, more specialized diagnostic tests are often even more appropriate. A urinalysis (U/A) is the simplest and least costly test that can provide a wealth of information. For the lower urinary tract, it is primarily used in the diagnosis of infection.
Although the abdominal radiograph known as a KUB (kidneys, ureters, and bladder) provides information regarding anatomy and may detect neoplasms or urinary stones, it is not the most frequently used procedure for this purpose. Ultrasonography, which is painless, does not involve radiation, and provides excellent visualization of the urinary system, is the most common initial screening study for infants and children with urinary problems. Cystography may be required to yield more specific information about the bladder than can be obtained by ultrasound.6 Voiding cystourethrography (VCUG) involves placing a catheter in the bladder and then filling it with sterile, iodinated, dilute contrast material. The catheter is then removed and the patient voids. Images of the bladder are taken before voiding to detect a ureterocele or tumor, and images taken during voiding can identify reflux or urethral abnormalities. Radionuclide voiding cystography also requires catheterization but involves the use of a small amount of radioactive material. A technetium-99m–labeled radiopharmaceutical is instilled in the bladder through the catheter, followed by sterile normal saline to fill the bladder. Once the catheter is removed, images are taken with the bladder full and during voiding, but this procedure does not allow visualization of the urethra.
The term urodynamic testing is used for procedures associated with diagnosing voiding dysfunction.6 There are multiple urodynamic tests and procedures and the choice of tests is based on clinical presentation and begins with the least invasive of the desired tests. The most common tests are cystometry (measurement of intrabladder pressure during filling); urethral pressure profilometry (measurement of intraluminal pressure along the length of the urethra); uroflowmetry (noninvasive method of measuring characteristics of urine flow); and pressure-flow micturition studies (invasive method of measuring characteristics of urine flow). Electrophysiologic testing may also be done to determine pathologic processes underlying voiding dysfunction. Neurophysiologic tests provide information about the coordination between the bladder and the external sphincter. Neurophysiologic tests are much more involved and are completed only in very specialized laboratories.
Physiology of Micturition
Micturition is often taken for granted by health care providers and patients, but is a complicated process. Understanding of the process begins with a review of the significant role the nervous system plays in controlling the functions of the lower urinary tract structures.
Nervous System Innervation of the Lower Urinary Tract
The central, autonomic, and peripheral nervous systems are all involved in urinary elimination. The pontine micturition center coordinates relaxation of the internal sphincter and contraction of the bladder to enable urination, whereas the cerebral cortex primarily inhibits the process through conscious control of the external sphincter.1 Any disease process affecting these areas can interfere with urination. This includes such pathologies as Parkinson disease, multiple sclerosis, traumatic brain injury, spinal cord injury, or stroke.
The smooth muscle of the bladder is innervated by both the sympathetic and parasympathetic branches of the autonomic nervous system (Figure 29-1). This innervation controls the detrusor muscle in the bladder wall and the bladder neck, ultimately controlling filling and emptying of the bladder. In other words, the bladder itself does not respond to voluntary control, but rather to neurologic reflexes. The nerves responsible for these reflexes have both autonomic efferent motor and afferent sensory roles; efferent nerves control bladder smooth muscle, and afferent fibers transmit sensations of bladder stretch—distention and fullness—and pain. Injury or disease of the spinal cord in this region profoundly affects lower urinary tract function.
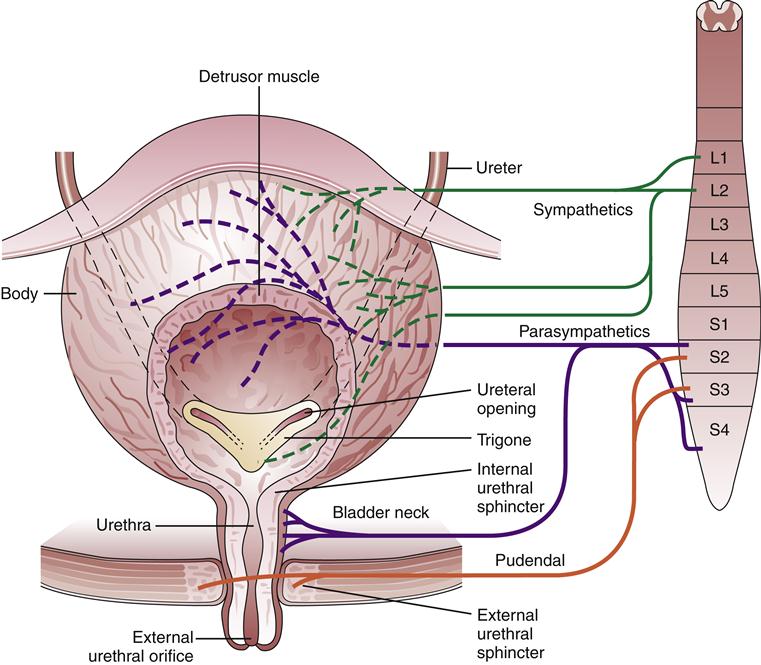
Sympathetic outflow of the autonomic nervous system to the bladder originates from the spinal cord region of L1-L2; the release of norepinephrine causes relaxation of the bladder and contraction of the bladder neck, allowing the storage of urine. Parasympathetic innervation of the urinary tract is supplied via the pelvic nerves, which exit the spinal cord at S2-S4. Their stimulation causes contraction of the detrusor muscle and relaxation of the internal sphincter (bladder neck). Parasympathetic signals from the posterior urethra in response to stretch of the bladder lining (urothelium) and bladder musculature are primarily responsible for initiating bladder emptying.
The somatic nerve fibers of the peripheral nervous system control the voluntary skeletal muscle of the external bladder sphincter via the pudendal nerve. The peripheral nervous system is primarily responsible for muscle function at the pelvic floor.
Mechanism of Micturition
The softness, pliability, mucosal secretions, and submucosal cushioning of the urethra are responsible for the maintenance of a water-tight seal or “compression” of the urethra. The internal sphincter is located at the proximal portion of the urethra, where the convergence of the detrusor muscle fibers provides pressure to keep it closed. When the internal sphincter has normal tone, the bladder is prevented from emptying until the pressure in the body of the bladder rises above a specific threshold. The sequence of urination begins with the bladder filling with urine until a first sensation of fullness is felt. This causes the internal bladder pressure to trigger stretch receptors in the bladder wall. Activation of these receptors results in afferent communication to the nervous system to cause contraction of the bladder detrusor muscle. The internal sphincter simultaneously relaxes, taking on a funnel shape.
The very noticeable urge to urinate causes an individual to consciously tighten the external sphincter. The external sphincter is located at the distal end of the urethra, surrounded by a ring of skeletal muscle from the pelvic floor. This musculature provides the necessary tension needed to maintain continence at normal resting bladder pressures. The external sphincter allows voluntary emptying of the bladder or the prevention of urination. Usually, enough pressure to hold the urine in the bladder can be voluntarily generated until about 350 to 400 ml of urine has collected in the bladder. At this point an urgent sensation to void occurs and the resulting activation of the voiding centers in the brain (central nervous system) also helps inhibit the bladder from emptying. At the appropriate time, a coordinated nerve response allows the detrusor muscle to contract and both urethral sphincters to relax, and voiding occurs. If an individual is able to coordinate urination at a suitable location and desired time, we consider the individual to be continent.
Normal adult bladder capacity is 300 to 500 ml; the urge to void usually develops when 150 to 250 ml are present.2 With an average fluid intake, this typically results in a voiding pattern of every 4 to 5 hours, with no need to awaken at night in order to void. With aging, bladder capacity declines to 200 to 350 ml; urination becomes more frequent (every 3 to 4 hours), and awakening at night to urinate is common. Under normal circumstances, the adult bladder contains less than 50 to 100 ml following voiding.2 This volume of postvoiding urine is called residual urine. Certain pathologies are associated with incomplete bladder emptying, and increased residual urine volumes.
Voiding Dysfunction
Voiding dysfunction can be associated with pathologies affecting the central, autonomic, and peripheral nervous systems. However, voiding dysfunctions may also be associated with other factors affecting control of micturition, including medications and access to toileting facilities. Disorders of the lower urinary tract, such as infection, can cause secondary problems with voiding. Voiding dysfunction encompasses several types of incontinence, and enuresis.
Incontinence
The International Continence Society defines the symptom of urinary incontinence as the report of any involuntary urine loss.7 Issues of urinary incontinence in adults are two times more common among women than men until age 80; after that point rates are equal.2 The prevalence of urinary incontinence increases across women’s lifetimes: 12% to 42% of middle-aged and younger women report urge incontinence, with these values increasing to 17% to 55% in older women.7 However, incontinence is not normal under any circumstances and is not a normal part of aging. In 2000 the overall cost of incontinence in the United States was nearly $20 billion.8 Itemization of these costs illustrates the complexity of the problem: 3% for diagnostic testing, 9% for routine care, 32% for treatments, and 56% for the indirect costs of nursing home admissions and loss of productivity.8 The personal financial cost is high as well; median weekly out-of-pocket costs for women with severe incontinence have been estimated at more than $10 in 2005 terms.9
Pathogenesis
Continence requires both physiologic and cognitive capabilities. Physiologic requirements include an appropriately functional nervous system, and intact bladder and urethral function. Cognitively, individuals must have the ability to react to bladder urges and be motivated to be continent. Any disruption in these capabilities can result in an inability to attain or maintain continence. Risk factors associated with acute and chronic urinary incontinence are listed in Box 29-1.
Urinary incontinence is not a part of normal aging, but it may be a result of disorders that are more common in the elderly or medications that induce urinary changes (e.g., diuretics). Age-related changes in the function or structure of the lower urinary tract and the possible limitations in the mobility and independence of the elderly predispose them to incontinence.8
Acute incontinence has a sudden onset and is due to potentially reversible, more easily treatable conditions. Examples of such conditions include urinary tract infections and constipation or fecal impactions.2 Chronic urinary incontinence is usually classified by type, based on the specific characteristics of presentation. These types are urge, stress, mixed, overflow, and functional incontinence. The etiologies and treatments vary, so identification of the type of incontinence is clinically important.
Stress incontinence, the most prevalent type of chronic incontinence, occurs when urine is involuntarily lost with increases in intraabdominal pressure.2,10 It is precipitated by effort or exertion, such as by lifting heavy objects, or by coughing or sneezing. Stress incontinence is thought to occur as a result of loss of pelvic muscle and/or fascial support of the bladder and urethra. Without this support, whenever there is an increase in intraabdominal pressure the normal angle between the bladder and posterior urethra is disrupted, forces that support urethral closure are reduced, and urine is lost.2,10 Decreased estrogen availability with menopause also contributes by reducing urethral closing pressure.11 Age-related loss of pelvic floor muscle fibers decreases muscular support. Other factors that favor the development of stress incontinence include obesity, childbirth-related trauma, urologic or retropubic surgery, pelvic radiotherapy, and the presence of conditions such as diabetes or degenerative neurologic diseases that impair nerves innervating the structures involved in micturition.2,10
Urge (urgency) incontinence involves the involuntary leakage of urine suddenly along with or immediately following the sensation of a need to urinate (urgency).7,12 This condition is most often due to an overactive detrusor muscle that suddenly contracts without the patient’s desire for it to do so.2 Aging is known to increase the frequency of spontaneous involuntary detrusor contractions.10 Contributing factors may include bladder infections that irritate the bladder lining and bladder outlet obstruction attributable to prostate enlargement. Urge incontinence is the most common type of incontinence experienced by older men.2 Additionally, urge incontinence may result from central nervous system conditions such as stroke, Parkinson disease, and multiple sclerosis in which damage to inhibitory pathways occurs. Finally, drugs that increase urine flow, such as diuretics and alcohol, can aggravate urge incontinence.10 In cases in which a specific cause is not determined, urge incontinence is said to be idiopathic. When urgency is associated with increased daytime frequency and nocturia (a need to get up at night to void), though not necessarily with incontinence, it is termed overactive bladder syndrome.12
Mixed incontinence is a combination of both stress and urge incontinence.7 It is common for these two types of incontinence to occur together, especially in older women. The self-report of mixed incontinence, as well as urge incontinence, has been associated with a greater impact on quality of life than the self-report of stress incontinence alone.5
Neurogenic bladder is a broad classification of voiding dysfunction in which the specific cause is a pathology that disrupts the nervous communication governing micturition. Patients with neurogenic bladder include those with central nervous system disorders (e.g., stroke, Parkinson disease, multiple sclerosis) and those with disorders affecting the autonomic innervation of the bladder (e.g., spinal cord injury, spinal cord anomalies such as meningocele). Depending upon the nature of the neurologic deficit, the result may be detrusor overactivity (spasticity) or hypotonia (flaccidity) of the bladder. Those affected may exhibit overflow incontinence, urge incontinence, uncoordinated detrusor contraction and urethral relaxation, or urinary retention.10 The phenomenon termed overflow incontinence occurs when the bladder becomes so full that it leaks urine, or “overflows.”8 This can also happen when an obstructed urethra prevents the bladder from emptying normally, such as with an enlarged prostate, urethral stricture, cystocele, or prolapsed uterus.
Some experts describe functional incontinence as incontinence related to physical or environmental limitations resulting in an inability to access a toilet in time.8 The urinary system may work well, but inaccessible toilets, mobility disorders, cognitive dysfunction, or mental disabilities prevent normal toilet usage. Health care workers can be critical in manipulating the environment to facilitate the patient’s timely access to the toilet to maintain “dependent continence.”12
Diagnosis
Patients should be assessed for reversible issues affecting the function of the lower urinary tract. These include potential drug-induced effects, UTIs or obstructions, fecal impaction, overuse of alcohol or caffeine, and excess intake of fluid. Impaired cognitive function may be due to chronic illness, depression, or delirium. All disorders associated with cognitive or neurologic function (e.g., stroke, Parkinson disease) should be identified. Circumstances or conditions affecting mobility should also be acknowledged.13
Patients may be asked to keep a bladder diary, recording the time, frequency, and volume of micturition as well as incidents of incontinence.7 In addition to the physical examination, such diagnostic tests as residual urine measurement, filling cystometry studies, and pressure flow studies during voiding may be used to establish the diagnosis of incontinence.6,7
Treatment
Management of incontinence begins by addressing reversible contributing factors. Lifestyle changes such as losing weight, reducing caffeine intake, and avoiding constipation may be useful. Additional treatment may include behavioral, pharmacologic, and surgical interventions, depending on the cause of incontinence. Pelvic floor muscle training (PFMT), a behavioral intervention, is recommended for urge incontinence in both men and women. PFMT may be as simple as the performance of exercises to strengthen pelvic muscles, or more complex to include techniques with vaginal weights, pelvic floor electrical stimulation, and biofeedback. Bladder training incorporates education, scheduled voiding with systematic delay of voiding to conform with the schedule, and positive reinforcement.
Pharmacologic agents may be used to promote or inhibit physiologic activities associated with micturition, depending on the cause of incontinence. This may include anticholinergic agents (e.g., oxybutynin), vaginal or oral estrogen, and α-adrenergic blockers (e.g., prazosin, tamsulosin) or 5α-reductase inhibitors (e.g., finasteride) for men with bladder outlet obstruction.14,15 The addition of drug therapy often increases the effectiveness of behavioral interventions. Injections with botulinum toxin are being used for detrusor overactivity. Surgical procedures for incontinence, used if nonsurgical interventions are ineffective, vary depending on the underlying anatomic or physiologic problems. Several surgical options are available to treat urge incontinence in women. The anterior colporrhaphy involves ther repair of a weakened anterior vaginal wall that has allowed the bladder to prolapse into the vagina. A colposuspension is performed by using sutures to tighten the muscles of the pelvic floor that support the uterus and bladder; the procedure may be performed via laparoscope. Sling procedures involve implanting strips of synthetic or natural material around the bladder neck and urethra to support urethral closure. Surgical options for men may include artificial urinary sphincter implantation for sphincter incompetence and placement of a perineal compression sling for post-prostatectomy incontinence.16
Incontinence that is not resolved by behavioral, pharmacologic, or surgical treatment occasionally may be managed by supportive approaches such as intermittent catheterization, indwelling catheterization, or use of incontinence undergarments.2 Each of these devices creates the potential for further complications. UTIs are more likely with stasis of urine in the bladder and, in the case of catheterization, with continuous or intermittent introduction of a foreign object into the normally sterile bladder. Catheterization is never an appropriate solution solely for caregiver convenience. Stasis of urine also increases the risk for bladder and renal calculi. Management of incontinence with incontinence undergarments predisposes patients to skin breakdown.
Enuresis
Enuresis as defined by the International Children’s Continence Society means intermittent incontinence while asleep.17 Nocturnal enuresis is a common childhood condition, more common in boys than girls. One study, conducted using a strict definition of enuresis as incontinence twice a week for a minimum of 3 consecutive months, estimated a prevalence of 4.45% in children in the United States ages 8 to 11.18 Primary nocturnal enuresis describes a child who has never achieved continence, whereas secondary enuresis refers to enuresis that develops after a period of at least 6 months of dryness.17 In monosymptomatic nocturnal enuresis, the child has nocturnal incontinence but no other signs of lower urinary tract malfunction such as urgency, postvoid dribbling, and daytime incontinence. Nonmonosymptomatic nocturnal enuresis is diagnosed when the child has symptoms of urgency, frequency, or daytime incontinence in addition to nighttime enuresis.
Pathogenesis
Primary monosymptomatic nocturnal enuresis is thought to be present in less than half of the cases of nocturnal enuresis.19 Three main mechanisms are considered to contribute to the condition. Some children exhibit nocturnal polyuria, linked in many cases to a deficiency in vasopressin (antidiuretic hormone [ADH]). Other children exhibit nocturnal overactivity of the detrusor muscle, which contributes to incontinence. Finally, immature or abnormal arousal mechanisms may explain why the child does not awaken.19,20
The fact that parents and siblings of children with nocturnal enuresis also report a history of the problem has led to the establishment of a genetic contribution.21 Enuresis is associated with such conditions as constipation, attention-deficit hyperactivity disorder, and sleep-disordered breathing.19,22,23
Diagnosis
Clinical workup for enuresis includes a thorough history of elimination patterns via a bladder diary and a physical examination to identify gross anatomic abnormalities. Children with monosymptomatic nocturnal enuresis (MNE) should also be tested for diabetes mellitus.19 Additional diagnostic tests, including flow cystometry and urinary tract imaging, are warranted for children who present with nonmonosymptomatic nocturnal enuresis (NMNE).24
Treatment
Treatment for MNE, not recommended before age 6, begins with education about appropriate daytime and bedtime voiding patterns.24 If constipation is present it is managed with fiber intake, physical activity, and stool softeners. Enuresis alarms, designed with a moisture sensor in the bed linen or nightclothes, arouse and/or condition children to contract pelvic muscles; alarm therapy is effective for approximately two thirds of children. A second course of alarm therapy may be required if there is relapse.19 “Overlearning” is recommended as a technique to strengthen the child’s response to a full bladder; after dryness is established the child is instructed to drink liquids an hour before bedtime.
Pharmacotherapy may be added if nonpharmacologic treatments are ineffective. Desmopressin, a vasopressin analogue, effects a full response in 30% of children and a partial response in 40%.19 Imipramine, a tricyclic antidepressant, is effective in about half of the children but its risk of cardiotoxicity mandates careful use in selected children. Anticholinergics such as oxybutynin and tolterodine are sometimes used, in combination with desmopressin or alone, and are effective in about 40% of cases. Urinary retention and constipation are side effects of anticholinergics that are worrisome in the setting of enuresis.19 In children who remain enuretic after many months of standard treatment, additional diagnostic testing such as ultrasound is recommended. Efforts to manage enuresis without treating an underlying pathology are likely to be unsuccessful.
Congenital Disorders
Vesicoureteral Reflux
Reflux of urine from the bladder to the ureter and renal pelvis, known as vesicoureteral reflux (VUR), is usually due to incompetence of the valvular mechanism at the ureter-bladder junction.
The incidence of vesicoureteral reflux in asymptomatic children (without a UTI) is low, estimated at 1%.25 However, the incidence in infants and children with UTIs is much greater, between 30% and 40%. More common in females, a genetic component is also present.26 In siblings of children in whom reflux had been diagnosed, the incidence is 27% to 51%. There is a 66% rate of VUR in the children of parents who have been diagnosed with reflux. The specific mode of inheritance has not yet been identified; a major, dominantly inherited allele, multifactorial or polygenic traits, and an X-linked pattern have all been postulated.27
Pathogenesis
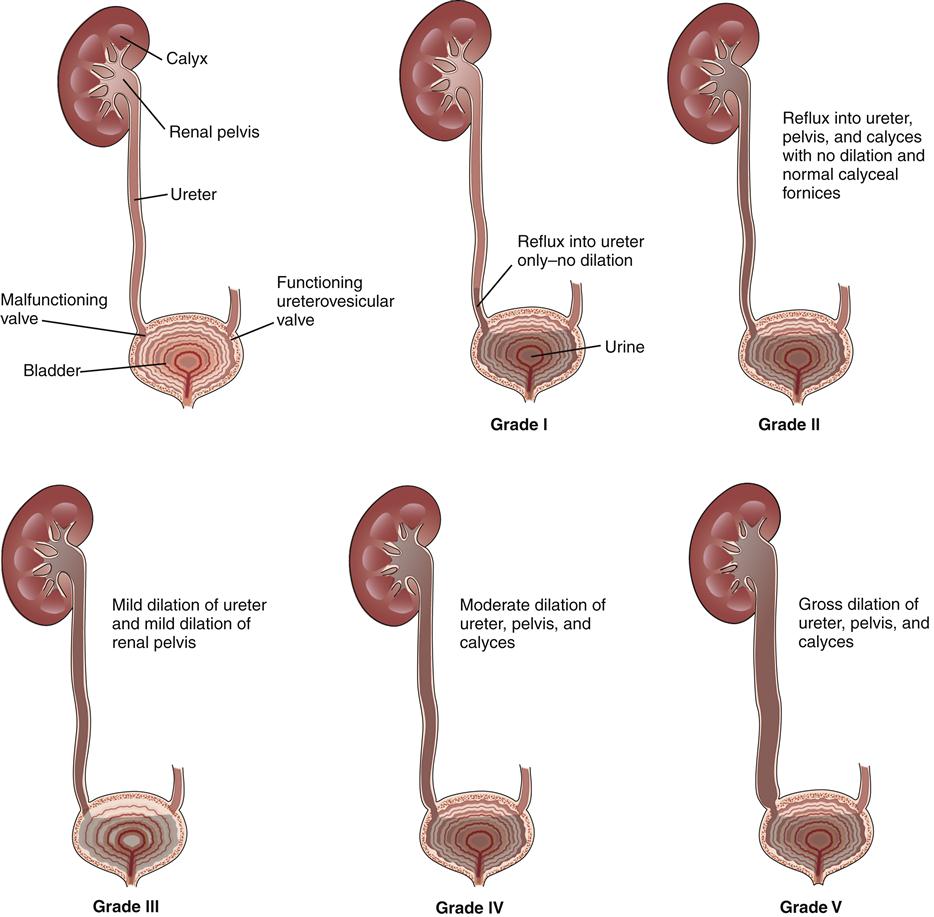
VUR is usually due to incompetence of the valvular mechanism at the ureter-bladder (ureterovesical) junction. Normally, the ureters enter the bladder at an oblique angle and then continue for 1 to 2 cm under the bladder mucosa before exiting inside the bladder cavity. As the bladder fills, pressure within it increases against the muscle wall and closes the ureteral passageway. In the case of VUR, closure of the ureteral passage is unsuccessful, and the urine flows backward into the ureters, sometimes reaching the kidney.
Vesicoureteral reflux is classified as being of either a primary or a secondary etiology. Congenital abnormalities at the ureterovesical junction are a chief cause of primary reflux.28 One such abnormality is a shortened ureteral tunnel through the bladder wall, which decreases the efficiency of the valvular mechanism. Impaired bladder dynamics may be a contributing factor; the prevalence reports of bladder dysfunction in children with primary VUR have ranged from 18% to 75%.28,29 Primary reflux is also associated with other abnormalities of the urinary system, among them ureteral duplication, ureterocele with duplication, ureteral ectopia, and paraurethral diverticula. Secondary reflux can occur from increased pressure within the bladder (neurogenic bladder, bladder outlet obstruction), inflammatory processes, or surgical procedures at or near the ureterovesical junction. Reflux may be bilateral or unilateral; the extent of reflux is graded from I to V (Figure 29-2).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


