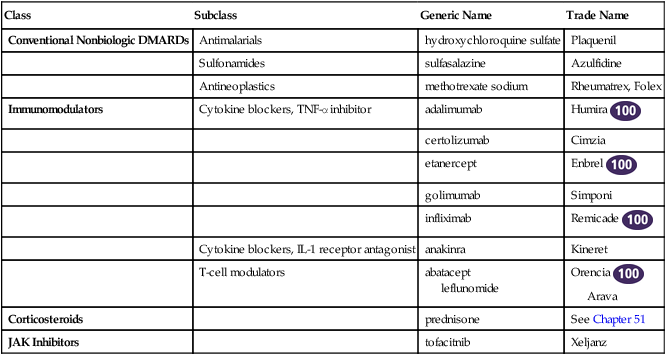
Chapter 37 INDICATIONS TABLE 37-1 Important Characteristics of DMARDs See Chapter 70, Immunizations and Biologicals, for discussion of the immune system.
Disease-Modifying Antirheumatic Medications and Immune Modulators
Class
Subclass
Generic Name
Trade Name
Conventional Nonbiologic DMARDs
Antimalarials
hydroxychloroquine sulfate
Plaquenil
Sulfonamides
sulfasalazine
Azulfidine
Antineoplastics
methotrexate sodium
Rheumatrex, Folex
Immunomodulators
Cytokine blockers, TNF-α inhibitor
adalimumab
Humira 
certolizumab
Cimzia
etanercept
Enbrel 
golimumab
Simponi
infliximab
Remicade 
Cytokine blockers, IL-1 receptor antagonist
anakinra
Kineret
T-cell modulators
abatacept
leflunomide
Orencia 
Arava
Corticosteroids
prednisone
See Chapter 51
JAK Inhibitors
tofacitnib
Xeljanz
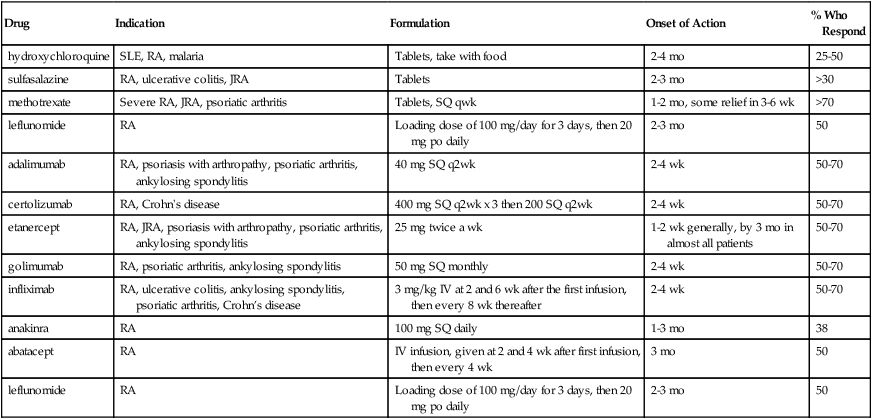
Drug
Indication
Formulation
Onset of Action
% Who Respond
hydroxychloroquine
SLE, RA, malaria
Tablets, take with food
2-4 mo
25-50
sulfasalazine
RA, ulcerative colitis, JRA
Tablets
2-3 mo
>30
methotrexate
Severe RA, JRA, psoriatic arthritis
Tablets, SQ qwk
1-2 mo, some relief in 3-6 wk
>70
leflunomide
RA
Loading dose of 100 mg/day for 3 days, then 20 mg po daily
2-3 mo
50
adalimumab
RA, psoriasis with arthropathy, psoriatic arthritis, ankylosing spondylitis
40 mg SQ q2wk
2-4 wk
50-70
certolizumab
RA, Crohn’s disease
400 mg SQ q2wk x 3 then 200 SQ q2wk
2-4 wk
50-70
etanercept
RA, JRA, psoriasis with arthropathy, psoriatic arthritis, ankylosing spondylitis
25 mg twice a wk
1-2 wk generally, by 3 mo in almost all patients
50-70
golimumab
RA, psoriatic arthritis, ankylosing spondylitis
50 mg SQ monthly
2-4 wk
50-70
infliximab
RA, ulcerative colitis, ankylosing spondylitis, psoriatic arthritis, Crohn’s disease
3 mg/kg IV at 2 and 6 wk after the first infusion, then every 8 wk thereafter
2-4 wk
50-70
anakinra
RA
100 mg SQ daily
1-3 mo
38
abatacept
RA
IV infusion, given at 2 and 4 wk after first infusion, then every 4 wk
3 mo
50
leflunomide
RA
Loading dose of 100 mg/day for 3 days, then 20 mg po daily
2-3 mo
50
Therapeutic Overview
Anatomy and Physiology
Mechanism of Action
Conventional DMARDs
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

 Top 100 drug.
Top 100 drug.
Full access? Get Clinical Tree


