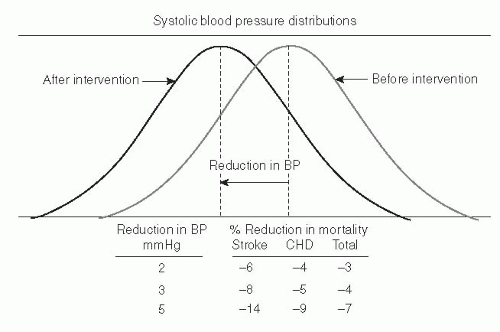
 Fig. 66.1. Estimated effects of population-wide shifts in systolic blood pressure (BP) on mortality. CHD, coronary heart disease. (Adapted with permission from Stamler R. Implications of the INTERSALT study. Hypertension 1991;17[Suppl]:I16-20.) |
States, roughly 69% of adults are considered either overweight or obese, as defined by a body mass index (BMI) of at least 25 kg/m2, and approximately 36% of adults are considered obese (BMI >30 kg/m2) (19). Among children and adolescents in the United States, the prevalence of obesity remains high (20). Concomitant with rising weight and the high prevalence of obesity in children are increased BP levels (21).
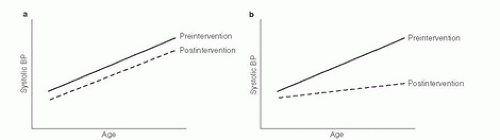 Fig. 66.2. A. Model in which a dietary intervention shifts age-blood pressure (BP) curve downward without affecting slope. B. Model in which a dietary intervention that shifts age-BP curve downward and reduces its slope. (Reprinted with permission from Appel LJ. Hypertension: A Companion to Braunwald’s Heart Disease. Philadelphia: Saunders, 2007:201-12.) |
TABLE 66.1 SUMMARY OF THE EVIDENCE ON THE EFFECTS OF DIETARY FACTORS AND DIETARY PATTERNS ON BLOOD PRESSURE | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 66.2 DIET-RELATED LIFESTYLE RECOMMENDATIONS | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
more than 50 randomized trials that have been performed to date. In a meta-analysis that focused on trials with plausible levels of sodium intake (30), a median reduction in urinary sodium of about 1.8 g/day (78 mmol/day) lowered SBP/DBP by 2.0/1.0 mm Hg in nonhypertensive individuals and by 5.0/2.7 mm Hg in hypertensive persons. A trial of 12 patients with resistant hypertension found that reducing sodium consumption by roughly 4500 mg/day lowered SBP/DBP by 22.7/9.1 mm Hg (31).
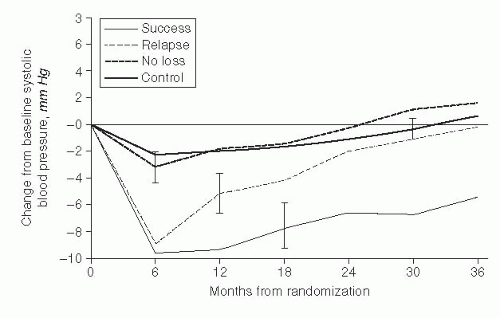 Fig. 66.3. Mean systolic blood pressure change in the Trials of Hypertension Prevention (TOHP2) in four groups of participants: those assigned to a weight loss group who successfully maintained weight loss, those assigned to a weight loss group who lost weight but experienced relapse, those assigned to a weight loss group who never lost weight, and the control group. (Reprinted with permission from Stevens VJ, Obarzanek E, Cook NR et al. Long-term weight loss and changes in blood pressure: results of the Trials of Hypertension Prevention, phase II. Ann Intern Med |
the setting of either the DASH diet (32) or a high dietary potassium intake.
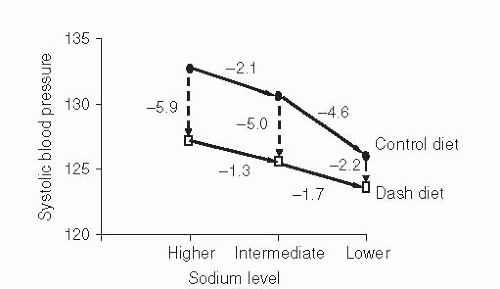 Fig. 66.4. Mean systolic blood pressure changes in the DASH-Sodium trial. The sample size was 412, 59% were prehypertensive, and 57% were African-American. Solid lines display the effects of sodium reduction in the two diets; hatched lines display the effects of the Dietary Approaches to Stop Hypertension (DASH) diet at each sodium level. (Adapted with permission from Sacks FM, Svetkey LP, Vollmer WM et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension [DASH] diet. DASH-Sodium Collaborative Research Group. N Engl J Med 2001;344:3-10.) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


