1. Describe the dematiaceous fungi, including natural habitat, transmission, and diseases with signs and symptoms. 2. Identify the site where mycetomas are frequently located and the population or populations at risk of infection. 3. Compare and contrast Exophiala jeanselmei and Exophiala dermatitidis, including test methods to distinguish between the two. 4. Describe the microscopic and morphologic features of Pseudallescheria boydii, including its sexual and asexual forms. 5. Differentiate the diagnostic microscopic features of the molds included in this chapter. Two types of mycetomas have been described. Actinomycotic (bacterial) mycetomas are caused by the aerobic actinomycetes, including Nocardia, Actinomadura, and Streptomyces spp. (The aerobic Actinomycetes are described in detail in Chapter 19.) Eumycotic (fungal) mycetomas are caused by a heterogeneous group of fungi that have septate hyphae. Eumycotic mycetomas are subcategorized as white grain mycetomas or black grain mycetomas, a distinction determined by the pigmentation of the infecting agent’s hyphae. The spectrum of disease caused by the dematiaceous fungi ranges from superficial infections (e.g., skin and hair) to emergent, rapidly progressive, and often fatal disease (e.g., brain abscess). The following list, which is not comprehensive, provides the common etiologic agents of diseases that may be caused by dematiaceous fungi (Table 61-1). TABLE 61-1 • Chromoblastomycosis: Cladosporium/Cladophialophora, Phialophora, and Fonsecaea spp. • Phaeohyphomycosis: E. jeanselmei; Exophiala dermatitidis; and Curvularia, Bipolaris, Alternaria, and Exserohilum spp. • Sinusitis: Alternaria, Bipolaris, Exserohilum, and Curvularia spp. • Mycotic keratitis and endophthalmitis: E. dermatitidis and Bipolaris and Curvularia spp. • Brain abscess: Cladophialophora bantiana, E. dermatitidis, and Bipolaris spp. See General Considerations for the Laboratory Diagnosis of Fungal Infections in Chapter 59. See General Considerations for the Laboratory Diagnosis of Fungal Infections in Chapter 59.
Dematiaceous (Melanized) Molds
Epidemiology and Pathogenesis
Superficial Infections (Tinea Nigra and Black Piedra)
Mycetoma
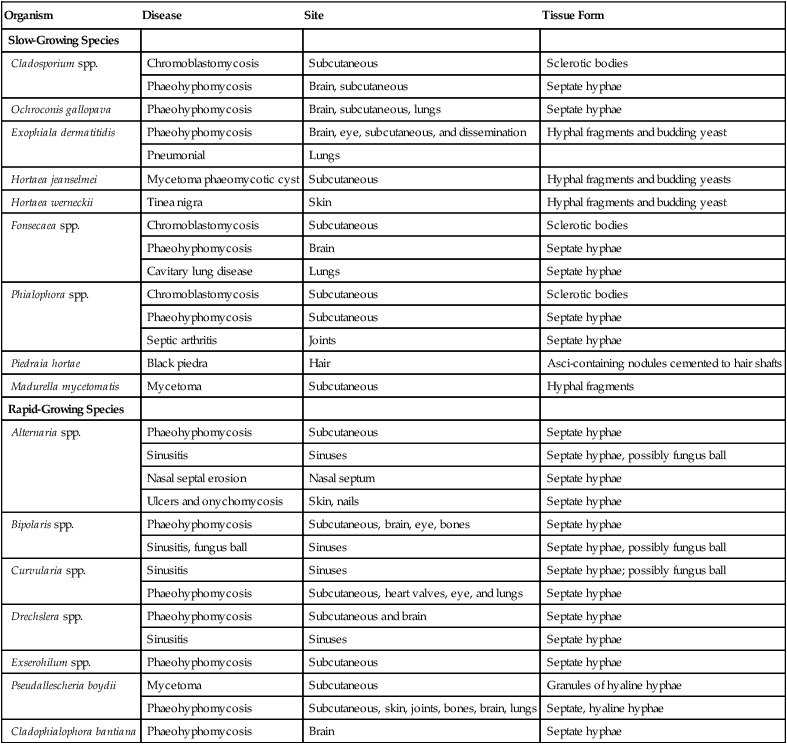
Pathogenesis and Spectrum of Disease
Organism
Disease
Site
Tissue Form
Slow-Growing Species
Cladosporium spp.
Chromoblastomycosis
Subcutaneous
Sclerotic bodies
Phaeohyphomycosis
Brain, subcutaneous
Septate hyphae
Ochroconis gallopava
Phaeohyphomycosis
Brain, subcutaneous, lungs
Septate hyphae
Exophiala dermatitidis
Phaeohyphomycosis
Brain, eye, subcutaneous, and dissemination
Hyphal fragments and budding yeast
Pneumonial
Lungs
Hortaea jeanselmei
Mycetoma phaeomycotic cyst
Subcutaneous
Hyphal fragments and budding yeasts
Hortaea werneckii
Tinea nigra
Skin
Hyphal fragments and budding yeast
Fonsecaea spp.
Chromoblastomycosis
Subcutaneous
Sclerotic bodies
Phaeohyphomycosis
Brain
Septate hyphae
Cavitary lung disease
Lungs
Septate hyphae
Phialophora spp.
Chromoblastomycosis
Subcutaneous
Sclerotic bodies
Phaeohyphomycosis
Subcutaneous
Septate hyphae
Septic arthritis
Joints
Septate hyphae
Piedraia hortae
Black piedra
Hair
Asci-containing nodules cemented to hair shafts
Madurella mycetomatis
Mycetoma
Subcutaneous
Hyphal fragments
Rapid-Growing Species
Alternaria spp.
Phaeohyphomycosis
Subcutaneous
Septate hyphae
Sinusitis
Sinuses
Septate hyphae, possibly fungus ball
Nasal septal erosion
Nasal septum
Septate hyphae
Ulcers and onychomycosis
Skin, nails
Septate hyphae
Bipolaris spp.
Phaeohyphomycosis
Subcutaneous, brain, eye, bones
Septate hyphae
Sinusitis, fungus ball
Sinuses
Septate hyphae, possibly fungus ball
Curvularia spp.
Sinusitis
Sinuses
Septate hyphae; possibly fungus ball
Phaeohyphomycosis
Subcutaneous, heart valves, eye, and lungs
Septate hyphae
Drechslera spp.
Phaeohyphomycosis
Subcutaneous and brain
Septate hyphae
Sinusitis
Sinuses
Septate hyphae
Exserohilum spp.
Phaeohyphomycosis
Subcutaneous
Septate hyphae
Pseudallescheria boydii
Mycetoma
Subcutaneous
Granules of hyaline hyphae
Phaeohyphomycosis
Subcutaneous, skin, joints, bones, brain, lungs
Septate, hyaline hyphae
Cladophialophora bantiana
Phaeohyphomycosis
Brain
Septate hyphae
 Bacterial: Nocardia, Actinomadura, and Streptomyces spp.
Bacterial: Nocardia, Actinomadura, and Streptomyces spp.
 White grain mycetoma: P. boydii and Acremonium and Fusarium spp.
White grain mycetoma: P. boydii and Acremonium and Fusarium spp.
 Black grain mycetoma: Madurella mycetomatis, Exophiala jeanselmei, and Curvularia spp.
Black grain mycetoma: Madurella mycetomatis, Exophiala jeanselmei, and Curvularia spp.
Laboratory Diagnosis
Specimen Collection and Transport
Specimen Processing
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine
