DPN Showing Wedge-Shaped Infiltrate This is a subtle case of deep penetrating nevus (DPN) on low-power examination. There are, however, dermally located subtle nests and fascicles of melanocytes . There is no junctional component.
DPN: Inflamed With Melanophages There is a lymphocytic infiltrate that surrounds the lightly melanized fascicles and nests of melanocytes . Note the melanophages located deep in the reticular dermis.
Melanocytes Intervening Between Collagen Bundles This power shows cords and smaller fascicles of melanocytes that intervene between collagen bundles. This feature may be more prominent in plexiform spindle cell tumors. It can resemble a dermatofibroma as the melanocytes “trap” collagen bundles .
Mild Cytological Atypia in DPN High-power examination shows mild, focal nuclear pleomorphism and prominent nucleoli . The remainder of nuclei are fusiform with smooth nuclear membranes and conspicuous nucleoli . No mitoses were found in this example.
TERMINOLOGY
Abbreviations
• Deep penetrating nevus (DPN)
Synonyms
• Plexiform spindle cell nevus
Definitions
• Benign, uncommon variant of melanocytic nevus (likely blue nevus variant)
Characterized by wedge-shaped or plexiform growth pattern
• Significant overlap with inverted type A nevus, but cytological atypia and low mitotic activity do not necessarily portend sinister outcome
• Clonal nevus may represent superficial variant of inverted type A nevus or DPN
ETIOLOGY/PATHOGENESIS
Histological Variance
• Often associated with 2nd nevoid subtype, thereby overlapping with combined nevus
• Variant of melanocytic nevi with histologic features that may be alarming and can be mistaken for malignant melanoma
CLINICAL ISSUES
Epidemiology
• Patients between 10-30 years
Site
• Head (face) and neck, back (upper trunk), and proximal extremities
Presentation
• Irregular dark brown to black papule or nodule measuring 0.2-1.0 cm in diameter
• Typically, they are darkly pigmented
• May show variegation in color, including shades of brown, blue, and black
Can create initial clinical concern for malignant melanoma (29% of cases)
Natural History
• Lesions without cytological atypia and low mitotic activity show no local recurrences and no distant metastases
• Those with atypia and mitotic activity > 3/mm² can metastasize
• DPN-like borderline tumors can be associated with regional lymph node metastasis
May exhibit potential for melanoma progression despite normal cytogenetic profile
Treatment
• Surgical approaches
When devoid of atypia, it is treated by simple excision
Patients with DPN-like borderline tumors should be aggressively managed
– At least complete reexcision and consideration of sentinel node biopsy, regardless of cytogenetic data
All atypical plexiform spindle cell melanocytic tumors should be completely excised with clear margins, and high-grade or potentially malignant lesions may require management as melanoma
Prognosis
• Patients with typical plexiform spindle cell melanocytic tumors do well
i.e., without tumor recurrence or death in mean follow-up period of 3.9 years
• 1 patient with atypical typical plexiform spindle cell melanocytic tumor had sentinel lymph node involvement
Patient was alive without recurrent disease at 1-year follow-up
• 3 patients with high-grade lesions developed lymph node involvement
All 3 patients were alive with 2-4 years of follow-up
• Patients with DPN-like borderline tumors may show lymph node involvement (33%)
Can rarely recur or metastasize
Only gold members can continue reading. Log In or Register to continue
 . There is no junctional
. There is no junctional  component.
component.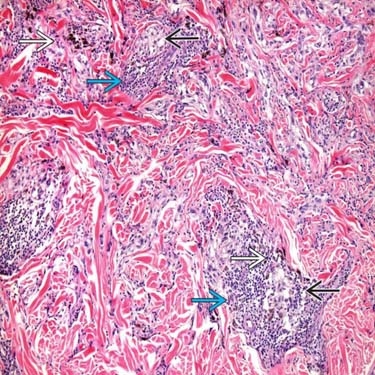
 that surrounds the lightly melanized fascicles and nests of melanocytes
that surrounds the lightly melanized fascicles and nests of melanocytes  . Note the melanophages
. Note the melanophages  located deep in the reticular dermis.
located deep in the reticular dermis.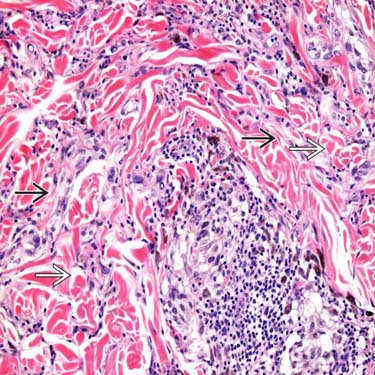
 that intervene between collagen bundles. This feature may be more prominent in plexiform spindle cell tumors. It can resemble a dermatofibroma as the melanocytes “trap” collagen bundles
that intervene between collagen bundles. This feature may be more prominent in plexiform spindle cell tumors. It can resemble a dermatofibroma as the melanocytes “trap” collagen bundles  .
.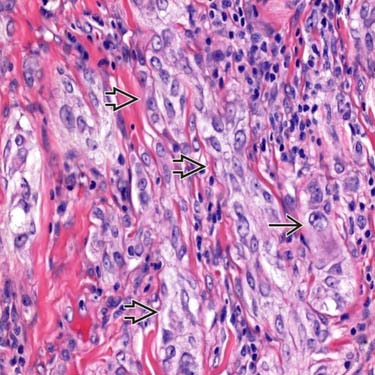
 . The remainder of nuclei are fusiform with smooth nuclear membranes and conspicuous nucleoli
. The remainder of nuclei are fusiform with smooth nuclear membranes and conspicuous nucleoli  . No mitoses were found in this example.
. No mitoses were found in this example.













