• Flow cytometry may underestimate number of plasma cells
• Plasmacytomas may show same molecular changes as seen in plasma cell myeloma
Top Differential Diagnoses
• Extranodal marginal zone lymphoma
• Reactive plasma cell infiltrates
Gross Image A single red solitary plaque on the forearm is shown, which microscopically is a cutaneous plasmacytoma (CP).
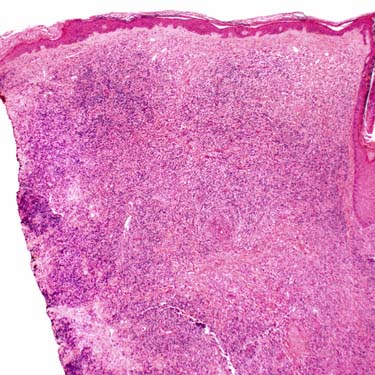
Low-Power of Cutaneous Plasmacytoma Low-magnification examination of a CP shows a diffuse, dermal-based lymphoid infiltrate with deep extension.
Higher Magnification of Cutaneous Plasmacytoma This CP shows a prominent plasmacytoid infiltrate surrounding multiple adnexal ducts and infiltrating between collagen bundles .
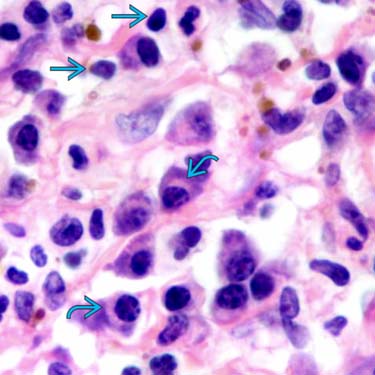
Plasma Cell Morphology This CP shows multiple mature-appearing plasma cells with prominent perinuclear hofs . Scattered small lymphocytes are also present.
TERMINOLOGY
Abbreviations
• Cutaneous plasmacytoma (CP)
Synonyms
• Extraosseous plasmacytoma of skin
Definitions
• Neoplasm of monoclonal plasma cells involving skin
Must exclude cutaneous involvement in multiple myeloma and plasmacytoid B-cell lymphomas, such as primary cutaneous extranodal marginal zone lymphoma
No clinical features of plasma cell myeloma and no evidence of bone marrow plasmacytosis
ETIOLOGY/PATHOGENESIS
Cell of Origin
• Clone of immunoglobulin-secreting, heavy-chain class-switched, terminally differentiated B cells that usually secrete single monoclonal immunoglobulin
CLINICAL ISSUES
Epidemiology
• Incidence
Extremely rare
– Only 3-5% of all plasma cell neoplasms
– Many cases previously reported as primary CPs would now be reclassified as extranodal marginal zone lymphomas
Rarely involve skin, more common in respiratory tract (80% of extraosseous plasmacytomas in oropharynx, nasopharynx, and nasal sinuses)
Rarely, may be seen as posttransplant lymphoproliferative disorder (PTLD)
– Morphologically identical to other plasmacytomas, but PTLD plasmacytoma-like tumors are often EBV(+)
• Age
Median age: 55 years
• Sex
Mostly in men; M:F = 2:1
Site
• Skin (by definition)
• Lesions may occur anywhere on body
Presentation
• Usually single or rarely multiple lesions
Upper airway/nasal lesions may present with rhinorrhea, nasal obstruction, epistaxis
Laboratory Tests
• Serum protein electrophoresis
20% reported to show monoclonal gammopathy
There is usually low level of M protein in serum &/or urine
Treatment
• Usually local radiation or surgery
Only gold members can continue reading. Log In or Register to continue

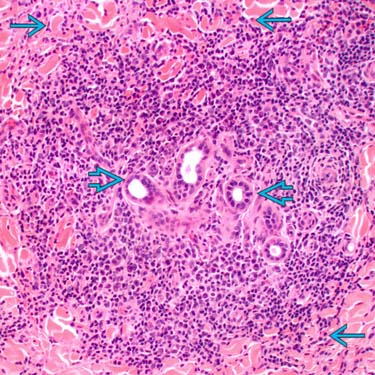
 and infiltrating between collagen bundles
and infiltrating between collagen bundles  .
.
 . Scattered small lymphocytes
. Scattered small lymphocytes  are also present.
are also present.












