Patient Story
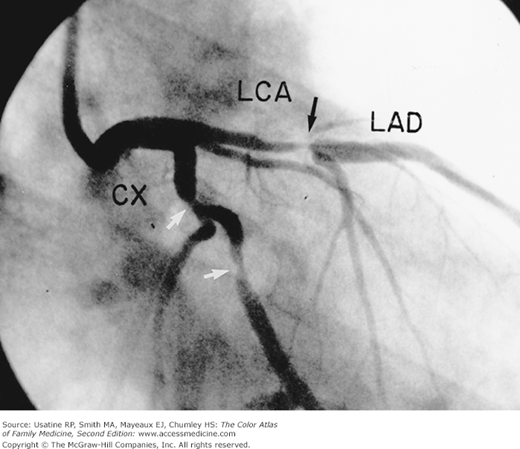
A 45-year-old man began having chest pressure with exertion that was relieved with rest. He did not have diabetes, high blood pressure, or high cholesterol, and had never had a myocardial infarction. His examination and resting ECG were normal. On the basis of the testing modalities available, he was scheduled for exercise stress testing. After a positive test, he underwent coronary angiography that demonstrated a significant stenosis in the left coronary artery (Figure 46-1). He underwent a stenting procedure and was placed on aspirin and cholesterol-lowering medication.

Introduction
In the United States, a person dies of coronary heart disease every 39 seconds. Coronary heart disease is a manifestation of atherosclerotic disease and has many modifiable risk factors. Patients with and without coronary heart disease should be advised to stop smoking, maintain normal blood pressure and cholesterol levels, exercise, achieve or maintain a normal weight, and control diabetes mellitus if present.
Epidemiology
- Coronary heart disease (CHD) is the leading cause of death in the United States, responsible for approximately 400,000 deaths in 2008.1
- Each year, 1.5 million myocardial infarctions occur (first and recurrent) with a 33% mortality rate.1
- In 2005, the prevalence of CHD among U.S. adults older than 18 years of age was higher in men than woman (8.2% vs. 5.0%) and higher in people with a less-than-high-school-diploma education (9.8% vs. 5.0% for college graduates).2
- In 2005, prevalence among white and black persons was similar.2
Etiology and Pathophysiology
- CHD is one of several manifestations of atherosclerotic disease, which begins with endothelium dysfunction.3
- Endothelium, when normal, balances vasoconstrictors and vasodilators, impedes platelet aggregation, and controls fibrin production.
- Dysfunctional endothelium encourages macrophage adhesion, plaque growth, and vasoconstriction by recruiting inflammatory cells into the vessel walls, the initiating step of atherosclerosis.
- The vessel wall lesions develop a cap of smooth muscle cells and collagen to become fibroadenomas.
- The vessels with these lesions undergo enlargement, allowing progression of the plaque without compromising the lumen.
- Plaque disruption and thrombus formation, instead of progressive narrowing of the coronary artery lumen, is responsible for two-thirds of acute coronary events.2
- Plaques most likely to rupture (high-risk plaques) have a large core of lipids, many macrophages, decreased vascular smooth muscle cells, and a thin fibrous cap.
- After plaque rupture, the exposed lipid core triggers a superimposed thrombus that occludes the vessel.
- Increased thrombosis is triggered by known cardiac risk factors including elevated low-density lipoprotein (LDL) cholesterol, cigarette smoking, and hyperglycemia.
- The other one-third of acute coronary events occurs at the site of very stenotic lesions (Figure 46-2).3
Risk Factors
- Family history of premature paternal or sibling myocardial infarction increases risk of heart disease by 50%.1
- Tobacco use and secondhand smoke exposure increase the risk of CHD and smoking cessation reduces risk.1
- High total cholesterol, high LDL, and/or low high-density lipoprotein (HDL) are independent risk factors.
- Physical inactivity has a relative risk of CHD of 1.5 to 2.4.1
- Overweight and obesity increases risk of heart disease by 20% (men and women) and 46% (men)/64% (women), respectively.1
- Diabetes mellitus increases risk of heart disease (hazard ratio 2.5).1
Diagnosis
- Typical angina is chest pain or pressure, brought on by exertion or stress, and relieved with rest or nitroglycerin.
- Atypical angina has two of the three features of typical angina; however, women with coronary artery disease report more neck, throat, or jaw pain.4
- Noncardiac chest pain has zero to one of the three features of typical angina.
- Risk factor assessment—Lipid profile and fasting blood glucose.
- Acute coronary syndrome—Cardiac-specific troponin is now preferred; when troponin cutoff is 0.1 g/L, sensitivity is 93%, specificity is 91%, positive likelihood ratio (LR+) is 10.33, and negative likelihood ratio (LR−) is 0.08.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


