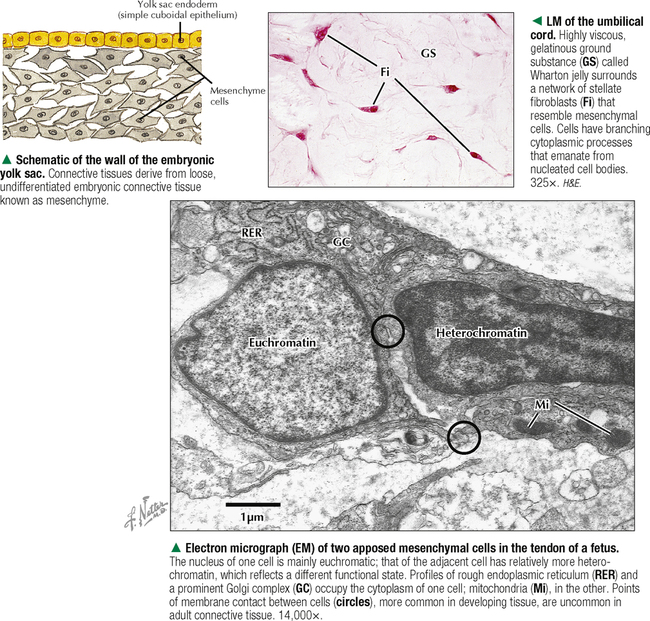
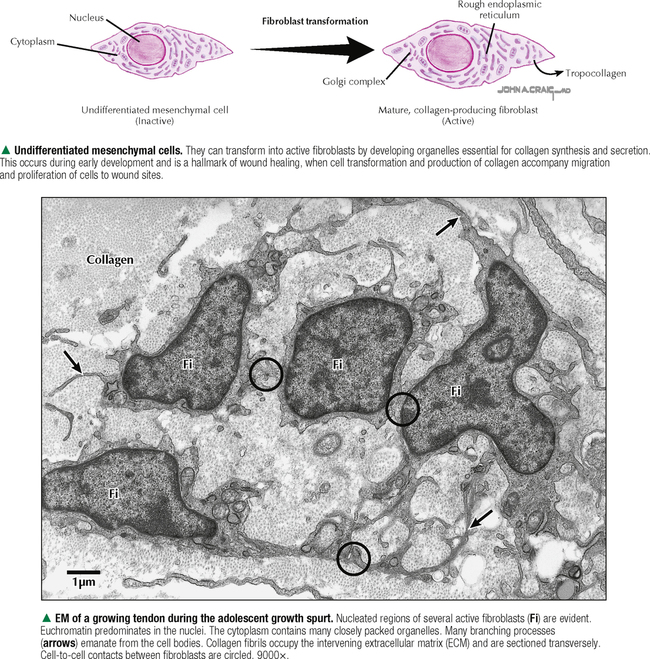
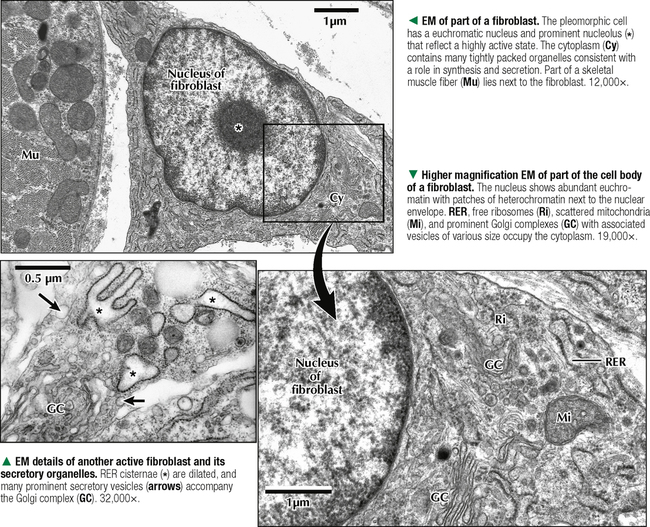
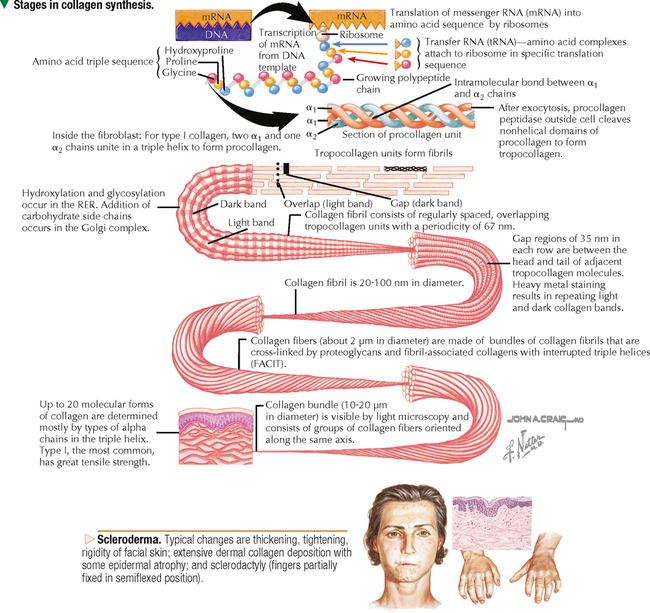
3 CONNECTIVE TISSUE 3.1. Overview 3.2. Classification of Connective Tissue Proper 3.3. Structure and Function of Mesenchymal Cells 3.4. Structure and Function of Fibroblasts 3.5. Ultrastructure and Function of Fibroblasts 3.6. Synthesis of Collagen 3.7. Types of Collagen and Its Ultrastructure 3.8. Histology of Elastic Connective Tissue 3.9. Histology of Reticular Connective Tissue 3.10. Histology and Function of Mast Cells 3.11. Ultrastructure and Function of Mast Cells 3.12. Histology and Function of Plasma Cells 3.13. Ultrastructure of Plasma Cells 3.14. Structure and Function of Macrophages 3.15. Ultrastructure and Function of Macrophages 3.16. Histology of Adipose Tissue 3.17. Ultrastructure and Function of Unilocular Adipocytes in White Fat 3.18. Ultrastructure and Function of Multilocular Adipocytes in Brown Fat 3.19. Histology of Tendons and Ligaments 3.1 OVERVIEW Adult connective tissue comprises a diverse family of tissues whose major function is to provide form and support to the body and organs and to connect and anchor parts. It is also a medium for exchange of nutrients, oxygen, and waste products between other tissues; it aids in defense and protection; and in certain sites, as in adipose tissue, it stores fat for cushioning and thermoregulation. Connective tissue, one of the four basic body tissues, is the most versatile, the types including connective tissue proper and the specialized blood, cartilage, and bone. Almost all connective tissue, regardless of form, arises embryonically from mesoderm; some connective tissue of the head originates from neural crest ectoderm. Like all body tissues, connective or supportive tissues consist of cells, both fixed and wandering, and an extracellular matrix (ECM) composed of fibers embedded in an amorphous ground substance. Cells of connective tissue include fibroblasts, mast cells, macrophages, plasma cells, adipocytes (fat cells), and pericytes. The many functions of connective tissue depend largely on the properties of the ECM, which predominates. Connective tissue proper includes a range of recognizable histologic types and can be classified as loose (areolar) or dense, mostly on the basis of the proportion and density of fibrous components of the ECM. Connective tissue may have a regular arrangement, as in a tendon, or an irregular arrangement, as in the dermis. CLINICAL POINT Mixed connective tissue disease (or Sharp syndrome)—an autoimmune disorder with overlapping features of lupus erythematosus, rheumatoid arthritis, systemic sclerosis, and polymyositis—occurs mostly in women and is usually diagnosed in young adults. There is genetic predisposition with familial occurrence, and patients have high serum titers of antinuclear and anti–U1-ribonuclear protein antibodies. Symptoms are fatigue, fever, joint swelling, and myositis. There is no cure, so treatment is targeted at suppressing immune-related tissue inflammation. Corticosteroids, when given early, can help symptoms. In some patients, clinical signs of this pattern illness may go into remission for several years and not need ongoing medication. Mild forms can be treated with nonsteroidal antiinflammatory drugs (NSAIDs) and antimalarial drugs. The prognosis is better than for other autoimmune diseases because of favorable response to corticosteroids. 3.2 CLASSIFICATION OF CONNECTIVE TISSUE PROPER The composition of connective tissues varies greatly in different parts of the body. On the basis of appearance and related to function, connective tissue proper can be placed into different categories in the adult and embryo. The main criteria are the amount and type of ECM, arrangement and kinds of fibers, and abundance and types of cells. Many classification schemes exist, but they represent a continuum of tissue types and, being arbitrary, should not be interpreted too rigidly. The two main types of adult connective tissue proper are loose (areolar) and dense. Loose connective tissue, the most widespread, has the greatest variety of cells and fibers. It is highly cellular with few fibers and has great flexibility. The term areolar refers to small fluid-filled spaces in this tissue. Much of the body’s tissue fluid is found within loose connective tissue, and excessive accumulation of this fluid causes swelling, or edema. Dense connective tissue has a greater proportion of fibers, fewer cells, and less ground substance. Its division into two subtypes depends on the orientation of its fibers. Dense irregular connective tissue has randomly oriented, interwoven fibers that can respond to stress in many directions. In dense regular connective tissue, fibers are in parallel and can withstand prolonged stress from one direction. Three specialized types of connective tissue in the adult are adipose, reticular, and elastic. The embryo and fetus have two types of connective tissue: Mesenchymal connective tissue occupies spaces between developing organs, and mucous connective tissue is in the umbilical cord. CLINICAL POINT Fibrosis is deposition and overgrowth of excess fibrous connective tissue that forms scar tissue because of injury, infection, allergy, or long-term inflammation. Fibrotic scarring is most common in the heart, lung, peritoneum, and kidneys. It differs from normal development of the stroma of organs and tissues because such scarring may obliterate normal architecture, leading to dysfunction and organ failure. Mechanisms of fibrosis include proliferation of fibroblasts, activation of macrophages and lymphocytes, and generation of novel cells (myofibroblasts) that, when activated, become the main collagen-producing cell. Many growth factors and cytokines that increase collagen synthesis, along with chemokines and angiogenic factors, are key regulators. Hence, such factors are potential targets of antifibrotic drugs for treatment of pulmonary fibrosis, hepatic cirrhosis, and Crohn disease. 3.3 STRUCTURE AND FUNCTION OF MESENCHYMAL CELLS Mesenchymal cells are primitive stem cells derived mostly from mesoderm or, in some sites, neural crest ectoderm. During embryonic development, they differentiate into various cell types for specific functions throughout the body; cells of connective tissue, bone, cartilage, blood, endothelium, and muscle derive from these undifferentiated cells. Also, some mesenchymal cells that retain plasticity persist in the adult and differentiate into diverse cell types when needed. Mesenchymal cells are often used as a source of pleuripotential stem cells for tissue repair and transplantation because they can develop into other cell types. Tissue remodeling in response to injury depends on mesenchymal cells that differentiate into fibroblasts and myofibroblasts, but it is unknown whether mesenchymal cells that participate in remodeling originate locally or from circulating precursor cells. Mesenchymal cells are normally inconspicuous in connective tissue. They resemble active fibroblasts but are usually smaller. They produce cytokines and growth factors that may significantly influence the differentiation and aging of other cells in the body such as those of epithelium and muscle. Unlike epithelial cells, mesenchymal cells can invade and migrate through the ECM to create important cell transpositions. They are common in walls of capillaries outside the endothelium where they are known as pericytes. CLINICAL POINT Tumors of connective tissue or its mesenchymal precursors are known as sarcomas. The most common adult soft tissue sarcoma is malignant fibrous histiocytoma. The cellular origin is uncertain, but immunocytochemical marker evidence indicates that it derives from perivascular mesenchymal cells. A gene associated with this tumor, MASL1, has been identified. Electron microscopy reveals a mixture of cells resembling fibroblasts, myofibroblasts, macrophages, and primitive mesenchymal cells. Tumors typically arise in deep fascia, soft tissues of the neck or extremities, and skeletal muscle. Distant metastasis may spread to lung, bone, or liver. Treatment is usually by radical resection. 3.4 STRUCTURE AND FUNCTION OF FIBROBLASTS Fibroblasts, the main cell type of connective tissue, are the most common cell of loose (areolar) connective tissue and virtually the only cell of dense regular connective tissue such as tendon. They function in synthesis and secretion of ground substance and, as their name implies, of connective tissue fibers, including collagen and elastic or reticular fibers, in the ECM. In mature connective tissue, these cells are relatively inactive and immobile and are often called fibrocytes. After injury and during wound repair, they rapidly proliferate and become active fibroblasts to synthesize new ECM fibers and ground substance. Fibroblasts are ovoid or stellate cells with long, tapering processes that branch. They have one elliptical nucleus, usually euchromatic, with one or more distinct nucleoli. Light microscopy shows that staining attributes of their cytoplasm differ according to functional state. Active or immature cells have a weakly basophilic, relatively conspicuous cytoplasm. Mature cells have a weakly acidophilic, barely visible cytoplasm with a relatively homogeneous appearance, so that nuclei are seen mainly in histologic sections. Routine preparations typically cannot resolve their cell borders, which are better shown by electron microscopy. 3.5 ULTRASTRUCTURE AND FUNCTION OF FIBROBLASTS Electron microscopic features of fibroblasts, which synthesize connective tissue fibers including collagen, are typical of most protein-synthesizing cells. Cell shape varies in different areas, but cells are usually elongated with many tapering cytoplasmic processes. The one elongated nucleus contains euchromatin, with clumps of heterochromatin next to the nuclear envelope. Active cells have one or two nucleoli and a cytoplasm rich in secretory organelles. A prominent Golgi complex and a pair of centrioles sit near the nucleus. Many small vacuoles and vesicles associated with the Golgi complex may contain flocculent material that consists of precursors of collagen and other extracellular substances produced by the cell. Oval to rod-shaped mitochondria are scattered in the cytoplasm. Cytoplasmic filaments, microtubules, and small vesicles associated with the cell surface are abundant. An extensive rough endoplasmic reticulum (RER) and free ribosomes dominate in actively secreting cells. The RER consists of rounded to flat cisternae studded with ribosomes. An important feature of connective tissue is an ability to provide repair after injury. Scars originate mainly from fibroblasts and their extracellular products. These cells have a capacity for regeneration throughout life. CLINICAL POINT Complex collagen synthesis can be impaired by dietary deficiency of vitamin C (ascorbic acid), producing scurvy, and by errors in critical genes or enzymes, leading to the rare Ehlers-Danlos syndrome (EDS). Lack of the vitamin causes nonhydroxylated, unstable collagen fibrils to fail to form a triple helix and have low tensile strength. Dentine (teeth), osteoid (bone), connective tissues, and tunica adventitia (blood vessel walls) are affected, but the typical hemorrhage and poor wound healing can occur anywhere. All of more than 10 forms of EDS involve a genetic defect in synthesis or assembly of collagen fibrils, the results being hyperelastic skin and hypermovable joints. Vascular EDS, the most severe, is caused by a COL3A1 gene mutation that leads to abnormal type III collagen. Serious effects include aortic rupture, colon perforation, and retinal detachment. 3.6 SYNTHESIS OF COLLAGEN Collagen formation involves both intracellular and extracellular events known in protein synthesis. Messenger RNA (mRNA) is synthesized from a template of DNA in the fibroblast nucleus. mRNA molecules enter the cytoplasm and attach to ribosomes of the RER. Ribosomes translate the nucleotide sequence of the mRNA into an amino acid sequence. A polypeptide chain of a specific sequence of several amino acids is assembled and then detaches from the ribosome to enter the RER cisternae. Hydroxylation of proline and lysine residues in the RER requires ascorbic acid (vitamin C) as a cofactor. Three alpha chains Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Like this:Like Loading… Related Related posts: CARDIOVASCULAR SYSTEM SPECIAL SENSES THE CELL FEMALE REPRODUCTIVE SYSTEM Stay updated, free articles. Join our Telegram channel Join Tags: Netters Essential Histology Jun 18, 2016 | Posted by admin in HISTOLOGY | Comments Off on CONNECTIVE TISSUE Full access? Get Clinical Tree
3 CONNECTIVE TISSUE 3.1. Overview 3.2. Classification of Connective Tissue Proper 3.3. Structure and Function of Mesenchymal Cells 3.4. Structure and Function of Fibroblasts 3.5. Ultrastructure and Function of Fibroblasts 3.6. Synthesis of Collagen 3.7. Types of Collagen and Its Ultrastructure 3.8. Histology of Elastic Connective Tissue 3.9. Histology of Reticular Connective Tissue 3.10. Histology and Function of Mast Cells 3.11. Ultrastructure and Function of Mast Cells 3.12. Histology and Function of Plasma Cells 3.13. Ultrastructure of Plasma Cells 3.14. Structure and Function of Macrophages 3.15. Ultrastructure and Function of Macrophages 3.16. Histology of Adipose Tissue 3.17. Ultrastructure and Function of Unilocular Adipocytes in White Fat 3.18. Ultrastructure and Function of Multilocular Adipocytes in Brown Fat 3.19. Histology of Tendons and Ligaments 3.1 OVERVIEW Adult connective tissue comprises a diverse family of tissues whose major function is to provide form and support to the body and organs and to connect and anchor parts. It is also a medium for exchange of nutrients, oxygen, and waste products between other tissues; it aids in defense and protection; and in certain sites, as in adipose tissue, it stores fat for cushioning and thermoregulation. Connective tissue, one of the four basic body tissues, is the most versatile, the types including connective tissue proper and the specialized blood, cartilage, and bone. Almost all connective tissue, regardless of form, arises embryonically from mesoderm; some connective tissue of the head originates from neural crest ectoderm. Like all body tissues, connective or supportive tissues consist of cells, both fixed and wandering, and an extracellular matrix (ECM) composed of fibers embedded in an amorphous ground substance. Cells of connective tissue include fibroblasts, mast cells, macrophages, plasma cells, adipocytes (fat cells), and pericytes. The many functions of connective tissue depend largely on the properties of the ECM, which predominates. Connective tissue proper includes a range of recognizable histologic types and can be classified as loose (areolar) or dense, mostly on the basis of the proportion and density of fibrous components of the ECM. Connective tissue may have a regular arrangement, as in a tendon, or an irregular arrangement, as in the dermis. CLINICAL POINT Mixed connective tissue disease (or Sharp syndrome)—an autoimmune disorder with overlapping features of lupus erythematosus, rheumatoid arthritis, systemic sclerosis, and polymyositis—occurs mostly in women and is usually diagnosed in young adults. There is genetic predisposition with familial occurrence, and patients have high serum titers of antinuclear and anti–U1-ribonuclear protein antibodies. Symptoms are fatigue, fever, joint swelling, and myositis. There is no cure, so treatment is targeted at suppressing immune-related tissue inflammation. Corticosteroids, when given early, can help symptoms. In some patients, clinical signs of this pattern illness may go into remission for several years and not need ongoing medication. Mild forms can be treated with nonsteroidal antiinflammatory drugs (NSAIDs) and antimalarial drugs. The prognosis is better than for other autoimmune diseases because of favorable response to corticosteroids. 3.2 CLASSIFICATION OF CONNECTIVE TISSUE PROPER The composition of connective tissues varies greatly in different parts of the body. On the basis of appearance and related to function, connective tissue proper can be placed into different categories in the adult and embryo. The main criteria are the amount and type of ECM, arrangement and kinds of fibers, and abundance and types of cells. Many classification schemes exist, but they represent a continuum of tissue types and, being arbitrary, should not be interpreted too rigidly. The two main types of adult connective tissue proper are loose (areolar) and dense. Loose connective tissue, the most widespread, has the greatest variety of cells and fibers. It is highly cellular with few fibers and has great flexibility. The term areolar refers to small fluid-filled spaces in this tissue. Much of the body’s tissue fluid is found within loose connective tissue, and excessive accumulation of this fluid causes swelling, or edema. Dense connective tissue has a greater proportion of fibers, fewer cells, and less ground substance. Its division into two subtypes depends on the orientation of its fibers. Dense irregular connective tissue has randomly oriented, interwoven fibers that can respond to stress in many directions. In dense regular connective tissue, fibers are in parallel and can withstand prolonged stress from one direction. Three specialized types of connective tissue in the adult are adipose, reticular, and elastic. The embryo and fetus have two types of connective tissue: Mesenchymal connective tissue occupies spaces between developing organs, and mucous connective tissue is in the umbilical cord. CLINICAL POINT Fibrosis is deposition and overgrowth of excess fibrous connective tissue that forms scar tissue because of injury, infection, allergy, or long-term inflammation. Fibrotic scarring is most common in the heart, lung, peritoneum, and kidneys. It differs from normal development of the stroma of organs and tissues because such scarring may obliterate normal architecture, leading to dysfunction and organ failure. Mechanisms of fibrosis include proliferation of fibroblasts, activation of macrophages and lymphocytes, and generation of novel cells (myofibroblasts) that, when activated, become the main collagen-producing cell. Many growth factors and cytokines that increase collagen synthesis, along with chemokines and angiogenic factors, are key regulators. Hence, such factors are potential targets of antifibrotic drugs for treatment of pulmonary fibrosis, hepatic cirrhosis, and Crohn disease. 3.3 STRUCTURE AND FUNCTION OF MESENCHYMAL CELLS Mesenchymal cells are primitive stem cells derived mostly from mesoderm or, in some sites, neural crest ectoderm. During embryonic development, they differentiate into various cell types for specific functions throughout the body; cells of connective tissue, bone, cartilage, blood, endothelium, and muscle derive from these undifferentiated cells. Also, some mesenchymal cells that retain plasticity persist in the adult and differentiate into diverse cell types when needed. Mesenchymal cells are often used as a source of pleuripotential stem cells for tissue repair and transplantation because they can develop into other cell types. Tissue remodeling in response to injury depends on mesenchymal cells that differentiate into fibroblasts and myofibroblasts, but it is unknown whether mesenchymal cells that participate in remodeling originate locally or from circulating precursor cells. Mesenchymal cells are normally inconspicuous in connective tissue. They resemble active fibroblasts but are usually smaller. They produce cytokines and growth factors that may significantly influence the differentiation and aging of other cells in the body such as those of epithelium and muscle. Unlike epithelial cells, mesenchymal cells can invade and migrate through the ECM to create important cell transpositions. They are common in walls of capillaries outside the endothelium where they are known as pericytes. CLINICAL POINT Tumors of connective tissue or its mesenchymal precursors are known as sarcomas. The most common adult soft tissue sarcoma is malignant fibrous histiocytoma. The cellular origin is uncertain, but immunocytochemical marker evidence indicates that it derives from perivascular mesenchymal cells. A gene associated with this tumor, MASL1, has been identified. Electron microscopy reveals a mixture of cells resembling fibroblasts, myofibroblasts, macrophages, and primitive mesenchymal cells. Tumors typically arise in deep fascia, soft tissues of the neck or extremities, and skeletal muscle. Distant metastasis may spread to lung, bone, or liver. Treatment is usually by radical resection. 3.4 STRUCTURE AND FUNCTION OF FIBROBLASTS Fibroblasts, the main cell type of connective tissue, are the most common cell of loose (areolar) connective tissue and virtually the only cell of dense regular connective tissue such as tendon. They function in synthesis and secretion of ground substance and, as their name implies, of connective tissue fibers, including collagen and elastic or reticular fibers, in the ECM. In mature connective tissue, these cells are relatively inactive and immobile and are often called fibrocytes. After injury and during wound repair, they rapidly proliferate and become active fibroblasts to synthesize new ECM fibers and ground substance. Fibroblasts are ovoid or stellate cells with long, tapering processes that branch. They have one elliptical nucleus, usually euchromatic, with one or more distinct nucleoli. Light microscopy shows that staining attributes of their cytoplasm differ according to functional state. Active or immature cells have a weakly basophilic, relatively conspicuous cytoplasm. Mature cells have a weakly acidophilic, barely visible cytoplasm with a relatively homogeneous appearance, so that nuclei are seen mainly in histologic sections. Routine preparations typically cannot resolve their cell borders, which are better shown by electron microscopy. 3.5 ULTRASTRUCTURE AND FUNCTION OF FIBROBLASTS Electron microscopic features of fibroblasts, which synthesize connective tissue fibers including collagen, are typical of most protein-synthesizing cells. Cell shape varies in different areas, but cells are usually elongated with many tapering cytoplasmic processes. The one elongated nucleus contains euchromatin, with clumps of heterochromatin next to the nuclear envelope. Active cells have one or two nucleoli and a cytoplasm rich in secretory organelles. A prominent Golgi complex and a pair of centrioles sit near the nucleus. Many small vacuoles and vesicles associated with the Golgi complex may contain flocculent material that consists of precursors of collagen and other extracellular substances produced by the cell. Oval to rod-shaped mitochondria are scattered in the cytoplasm. Cytoplasmic filaments, microtubules, and small vesicles associated with the cell surface are abundant. An extensive rough endoplasmic reticulum (RER) and free ribosomes dominate in actively secreting cells. The RER consists of rounded to flat cisternae studded with ribosomes. An important feature of connective tissue is an ability to provide repair after injury. Scars originate mainly from fibroblasts and their extracellular products. These cells have a capacity for regeneration throughout life. CLINICAL POINT Complex collagen synthesis can be impaired by dietary deficiency of vitamin C (ascorbic acid), producing scurvy, and by errors in critical genes or enzymes, leading to the rare Ehlers-Danlos syndrome (EDS). Lack of the vitamin causes nonhydroxylated, unstable collagen fibrils to fail to form a triple helix and have low tensile strength. Dentine (teeth), osteoid (bone), connective tissues, and tunica adventitia (blood vessel walls) are affected, but the typical hemorrhage and poor wound healing can occur anywhere. All of more than 10 forms of EDS involve a genetic defect in synthesis or assembly of collagen fibrils, the results being hyperelastic skin and hypermovable joints. Vascular EDS, the most severe, is caused by a COL3A1 gene mutation that leads to abnormal type III collagen. Serious effects include aortic rupture, colon perforation, and retinal detachment. 3.6 SYNTHESIS OF COLLAGEN Collagen formation involves both intracellular and extracellular events known in protein synthesis. Messenger RNA (mRNA) is synthesized from a template of DNA in the fibroblast nucleus. mRNA molecules enter the cytoplasm and attach to ribosomes of the RER. Ribosomes translate the nucleotide sequence of the mRNA into an amino acid sequence. A polypeptide chain of a specific sequence of several amino acids is assembled and then detaches from the ribosome to enter the RER cisternae. Hydroxylation of proline and lysine residues in the RER requires ascorbic acid (vitamin C) as a cofactor. Three alpha chains Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Like this:Like Loading… Related Related posts: CARDIOVASCULAR SYSTEM SPECIAL SENSES THE CELL FEMALE REPRODUCTIVE SYSTEM Stay updated, free articles. Join our Telegram channel Join Tags: Netters Essential Histology Jun 18, 2016 | Posted by admin in HISTOLOGY | Comments Off on CONNECTIVE TISSUE Full access? Get Clinical Tree