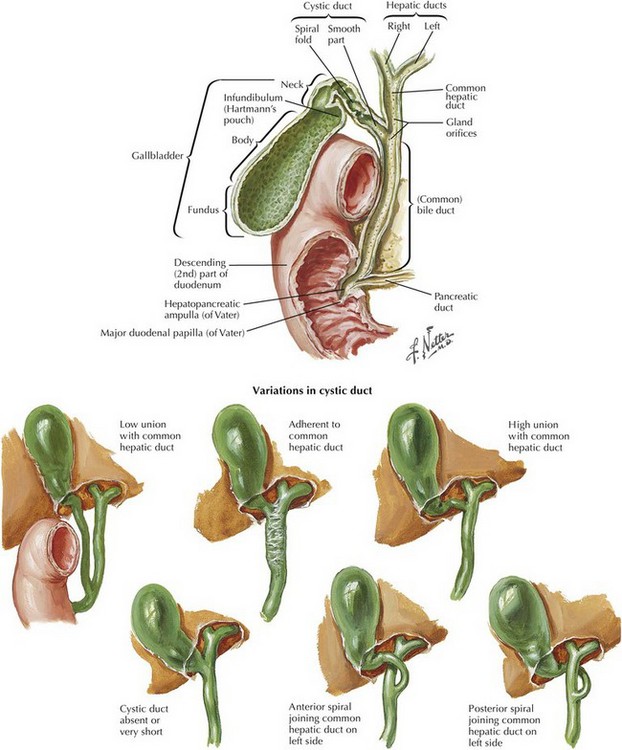
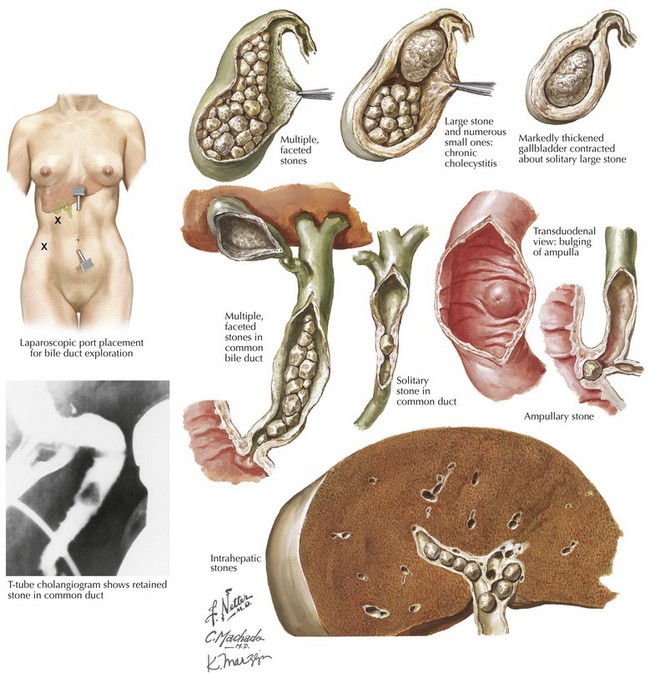
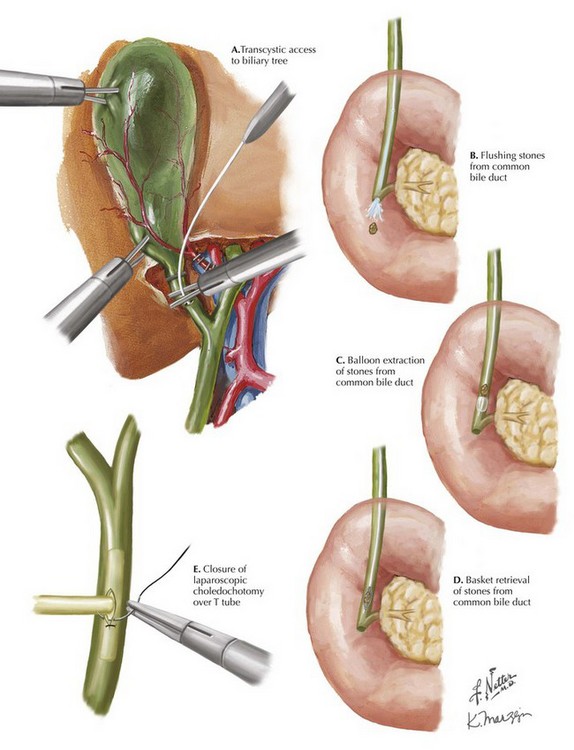
Chapter 13 In most individuals (64% to 75%) the cystic duct joins the hepatic duct at approximately a 40-degree angle (Fig. 13-1). Less frequently (17% to 23%) the cystic duct runs parallel to the hepatic duct for a distance and may even enter the duodenum separately. In 8% to 13% of individuals the cystic duct may enter the hepatic duct on the left side after passing in front of or behind the common hepatic duct. Infrequently, the gallbladder may be sessile, with little to no cystic duct. If CBD stones are identified at laparoscopic cholecystectomy, laparoscopic CBD exploration may be warranted (Fig. 13-2). Successful laparoscopic CBD exploration avoids the risks associated with deferring treatment of a CBD stone or a subsequent endoscopic procedure. The transcystic approach to CBD exploration avoids a choledochotomy and eliminates the subsequent need for a T tube. After controlling the cystic duct on the gallbladder side, a cystic ductotomy is created and a cholangiocatheter placed. The cystic duct may need to be dilated with a balloon before subsequent interventions to extract calculi (Fig. 13-3, A).
Common Bile Duct Surgery and Choledochoduodenostomy
Cystic Duct Anatomy and Variants
Laparoscopic Common Bile Duct Exploration
Transcystic Approach
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Common Bile Duct Surgery and Choledochoduodenostomy