Patient Stories
A 1-month-old child was seen in the emergency room for bruising. Physical examination revealed bruises to the buttocks, chest, and eye. The parents reported that the child received the buttock bruise (Figure 8-1) after being dropped by the father, that the chest bruise was from the child’s seat belt, and the eye bruise from accidentally hitting the child with an elbow while cosleeping. The social worker was consulted in the emergency room, and found no concerning “red flags” in the family. The emergency room physician felt the findings were because of inexperienced parents. The child was sent home with the parents, and the emergency room later reported the case to Children’s Protective Services (CPS) in hopes of providing the family with support services. A child abuse pediatrician (CAP) was consulted by CPS to review the case the next day. The CAP requested that the child be brought back to the hospital emergently for further evaluation. A skeletal survey, including oblique views of the ribs, at that time showed a healing fracture of the eighth posterior rib (Figure 8-2). A head CT and liver function tests were performed to screen for occult trauma, and laboratory tests were done to evaluate for a bleeding diathesis. All were negative. Law enforcement was contacted and coinvestigated with CPS. The child was placed in the home of a relative. Two weeks later, a repeat skeletal survey showed new bone formation over the right femur, indicating a healing fracture.

Figure 8-2
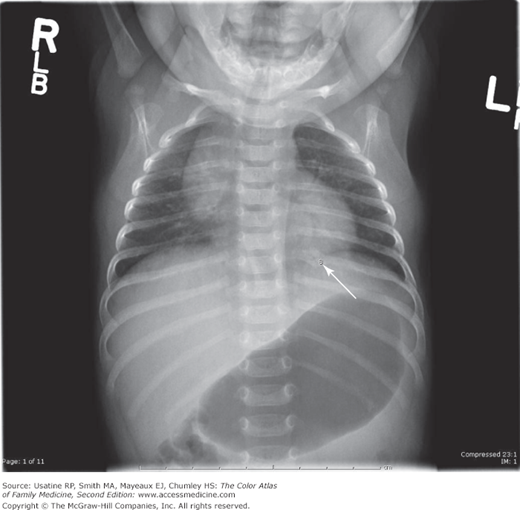
Healing eighth posterior rib fracture in the same child from Figure 8-1. A skeletal survey is indicated in any child younger than 2 years of age where suspicions of physical abuse exist. (Courtesy of James Anderst, MD, MS.)
A 15-month-old child is brought to the emergency department by the police after a relative called 911. The child and his mother attended a family gathering where concerned relatives viewed the mother’s story that the child “falls a lot” with suspicion. On examination there were many signs of physical abuse (Figures 8-3, 8-4, and 8-5). His face was covered with bruises, especially around the right eye and cheek (Figure 8-3). His axilla showed signs of being gouged with fingernails (Figure 8-4). Although an initial skeletal survey did not show any fractures, a repeat skeletal survey and oblique views of the ribs were done 2 weeks later. The second skeletal series showed eight healing rib fractures. Repeat skeletal surveys are recommended in children younger than 4 years of age, who are confirmed or suspected victims of abuse (Figure 8-5). The child was admitted to the hospital and the police, hospital social workers, and CPS were notified. In the emergency department, the child was evaluated by a forensic nurse examiner trained in child-abuse photo documentation. The child was then referred to a CAP who assessed mechanisms of injuries, reexamined the child, and interpreted the initial and follow-up skeletal surveys.
Figure 8-3

A 15-month-old boy who has been physically abused by his mother’s boyfriend for several weeks. There is bruising under both eyes, with the greatest degree of bruising seen under the right eye and on the right cheek. The boy is in the emergency department after concerned relatives called the police. (Courtesy of James Anderst, MD, MS.)
Figure 8-4

Same 15-month-old boy from Figure 8-3 with multiple fingernail gouges in his right axilla. Some are fresh and one appears to be older and somewhat crusted. Injuries in different stages of healing may indicate chronicity of abuse. (Courtesy of James Anderst, MD, MS.)
Figure 8-5
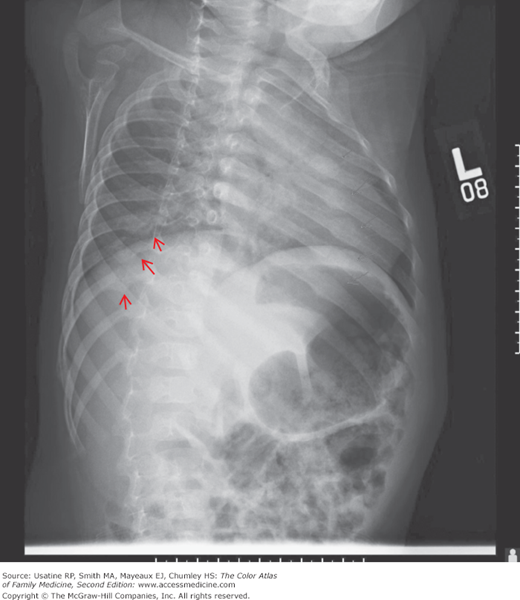
Same boy from Figure 8-3 with oblique X-ray showing healing rib fractures with callus in eight different locations as marked by the arrows. The degree of callus formation shows that these rib fractures are not new. Oblique radiographs should be requested in addition to a “skeletal survey” because lateral rib fractures are best seen with this view. (Courtesy of James Anderst, MD, MS.)
Introduction
The appropriate identification of child physical abuse is critical. Misdiagnoses in either direction (missed abuse or inappropriate diagnosis of abuse) are extremely harmful to the child and family. A careful evaluation of each case, coupled with an application of the existing scientific data on child physical abuse, may result in improved outcomes for the child and family.
Epidemiology
- Occurs in 9.2 per 1000 children, with highest rate of victimization in the birth to 1 year age group (20.6 per 1000).
- The Department of Health and Human Services compilation of State CPS Child Maltreatment 2010 had 3.3 million CPS reports filed in 2010, with 695,000 confirmed child victims.1 Of these:
- Seventy-eight percent were neglected.
- Eighteen percent were physically abused.
- Nine percent were sexually abused.
- Eight percent were psychologically abused.
- Seventy-eight percent were neglected.
- Nearly 81% of victims were abused by a parent acting alone or with another person.
- Medical personnel made only 8.2% of the referrals to CPS.
Risk Factors
Diagnosis
- History inconsistent with child’s developmental stage.
- Injuries inconsistent with history given.
- History changes over time.
- History differs among witnesses.
- Delay in seeking medical care (must consider family’s access to care and availability of transportation).
- Sibling blamed.
- Magical injury—No one knows how it happened.
- Bruising:6
- In children who are not independently mobile.
- Seen away from boney prominences.
- To the face, hands, ears, buttocks, back, abdomen, and arms.
- In the shape of an imprint of an object or hand, or a ligature (Figure 8-6).
- Multiple bruises in clusters.
- In children who are not independently mobile.
- Burns:7
- Inconsistent with history (Figure 8-7).
- Stocking/glove distribution.
- Well-demarcated edges.
- Symmetrical burns.
- No splash marks.
- Inconsistent with history (Figure 8-7).
- Fractures:8
- Rib fractures.
- Fractures in immobile children that are not attributable to birth injury.
- Multiple fractures and/or multiple fractures of different ages.
- Fractures in the absence of a history of trauma.
- Any fracture that is inconsistent with the reported mechanism.
- Rib fractures.
- Intracranial injury:
- Highly variable clinical presentation, however presence of apnea, retinal hemorrhages, and/or rib fractures is more strongly associated with inflicted (versus noninflicted) intracranial injury.9,10
- Mild abusive head injury may present with isolated vomiting or fussiness.11

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


- Highly variable clinical presentation, however presence of apnea, retinal hemorrhages, and/or rib fractures is more strongly associated with inflicted (versus noninflicted) intracranial injury.9,10
