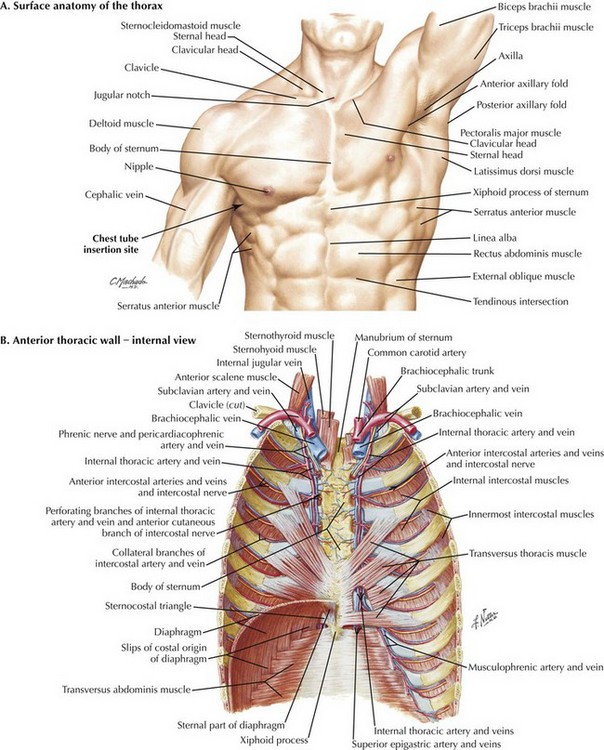
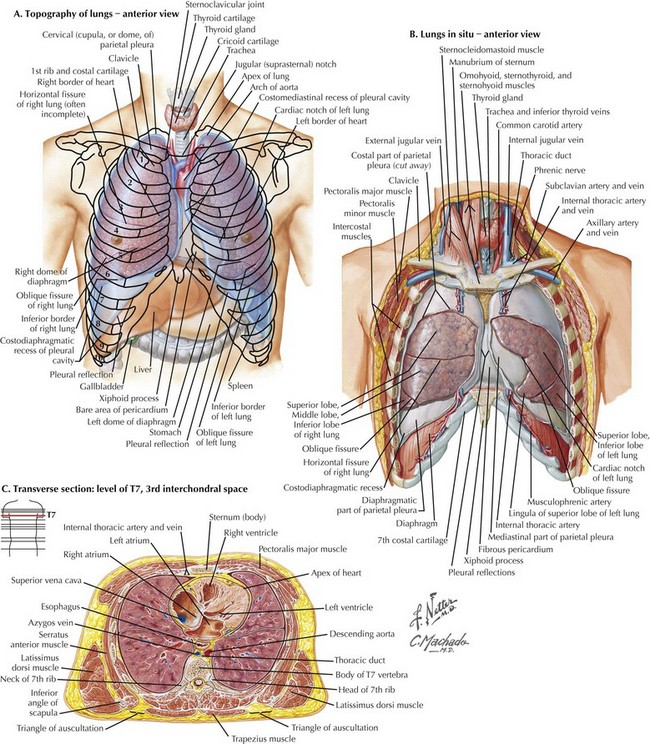
Chapter 43 1. Identification of superficial landmarks 2. Relationship of the ribs and neurovascular bundle 3. Recognition of the boundaries of the chest and pleural space 4. Differences between right and left chest 5. Cross-sectional anatomy to visualize layers of the chest wall The first important concept of placing a chest tube or accessing the pleural space involves the ability to identify superficial anatomic landmarks (Fig. 43-1, A). The key landmarks for accessing the pleural space are identification of the clavicular head; midclavicular line; the anterior, middle, and posterior axillary lines; and intercostal spaces with corresponding ribs. The ability to count ribs accurately will facilitate the placement of chest tubes. In a female patient the nipple should not be used as a landmark. Instead, the inframammary fold should be used to identify the 5th rib at the anterior axillary line. In a male patient the lower border of the pectoralis major muscle is a good approximation for the site of tube insertion. The second key concept when accessing the pleural space is to recognize that the intercostal neurovascular bundles lie just below the inferior portion of the ribs (Fig. 43-1, B). Thus it is important to place the chest tube over the most superior portion of the rib to avoid injuring the intercostal neurovascular bundle. The third anatomic principle is to recognize the boundaries of the chest and pleural space. Failure to recognize these boundaries can result in misadventures in chest tube placement such as placing a tube into or below the diaphragm, which can cause bleeding or injury to intraabdominal or major vascular structures (Fig. 43-2, A).
Chest Tube Placement
Superficial Anatomy and Topographic Landmarks
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine