Endogenous commensal that is part of normal flora of GI tract, mouth, respiratory tract, vagina
• Risk factors include disruption of mucosal or cutaneous barriers, immunosuppression, use of broad-spectrum antibiotics
Clinical Issues
• Presentation may be very nonspecific (fever, hepatomegaly, abdominal pain)
• Prognosis depends on underlying immune status of patient
Macroscopic
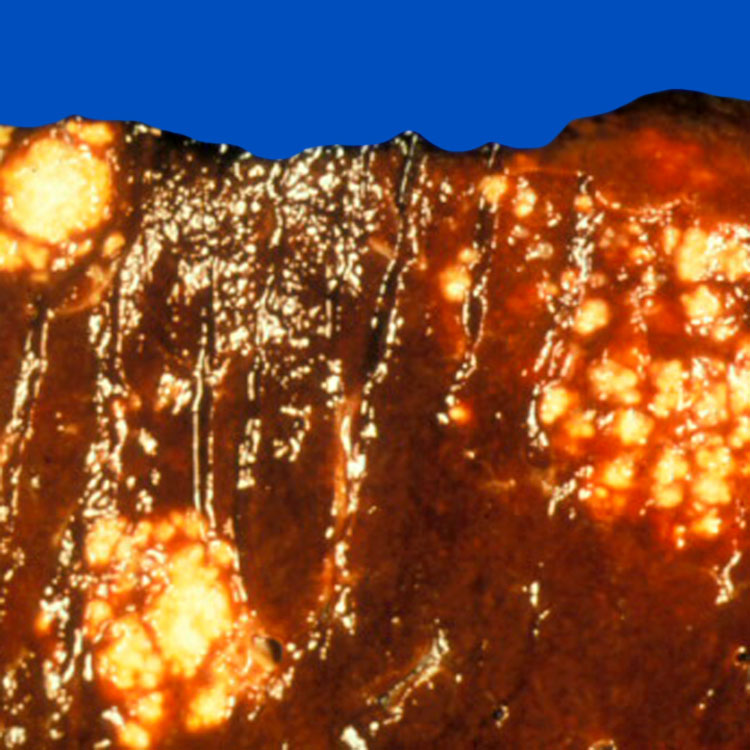
• Yellow-white nodules
Usually multiple, 1-2 cm
Microscopic
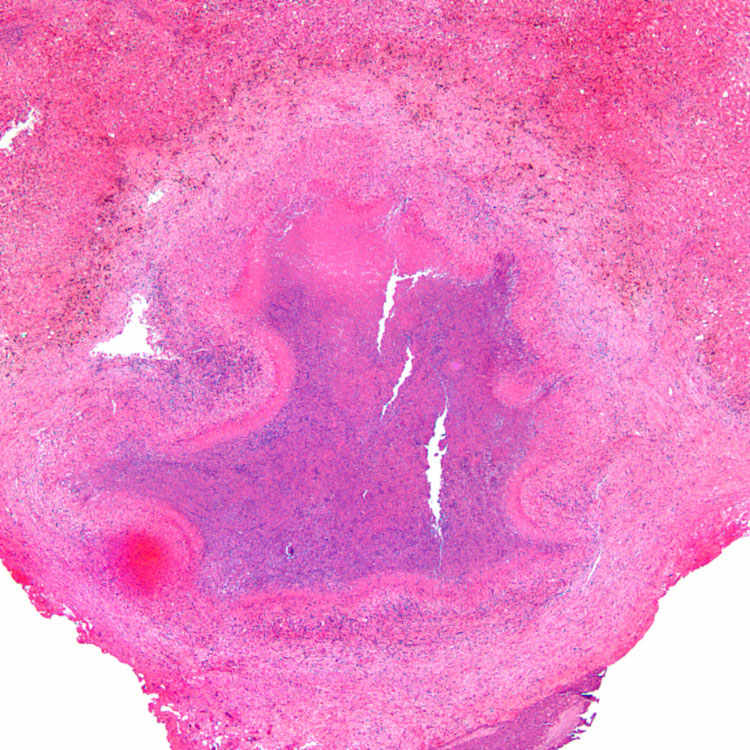
• Typical inflammatory reaction is granulomatous
Frequently with suppurative/necrotic center
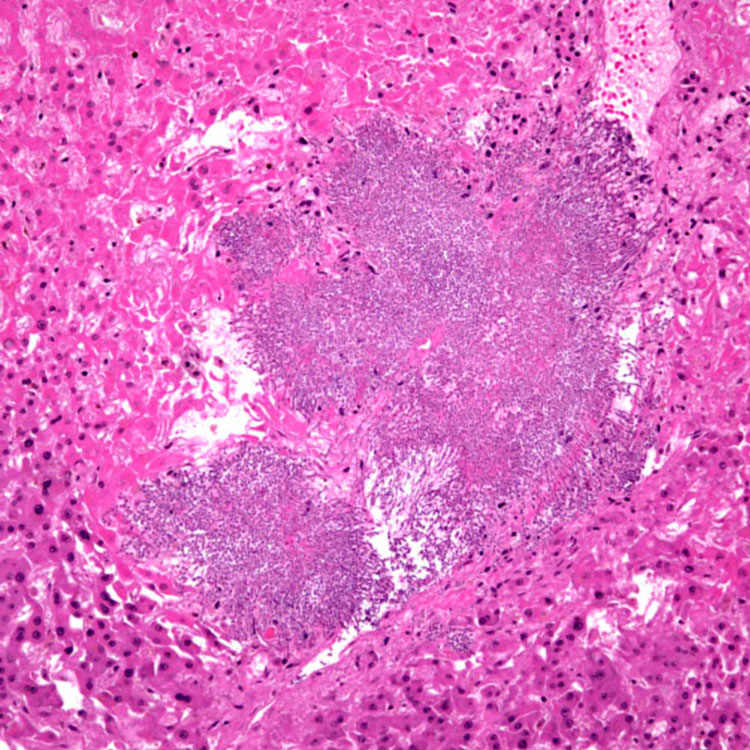
May have minimal inflammation in severely immunocompromised patients
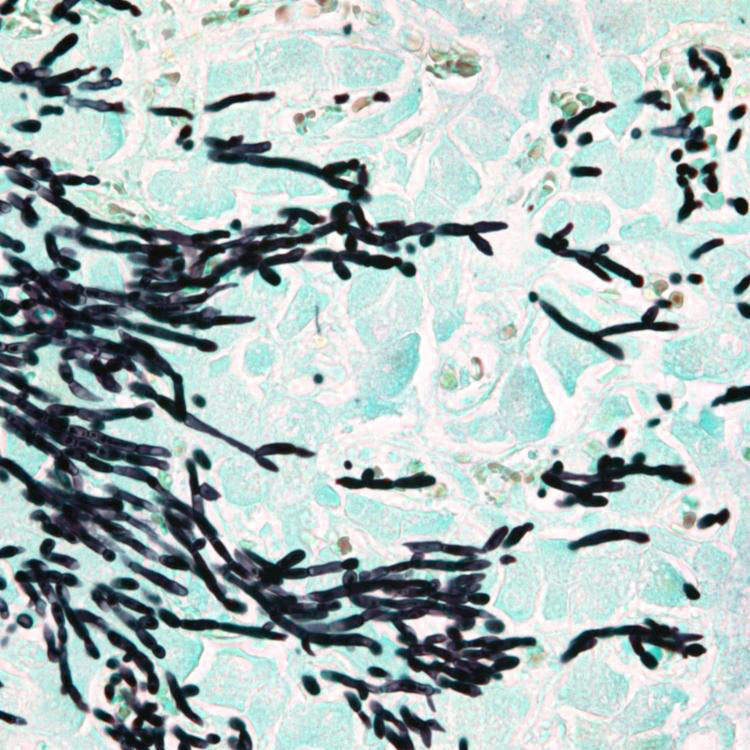
• Mixture of budding yeast, hyphae, and pseudohyphae
GMS, PAS positive
Ancillary Tests
• PCR
• Culture
Diagnostic Checklist
• Fungi can sometimes be speciated by morphology but need confirmatory test
Gross Appearance Gross photograph shows a liver from an autopsy showing multiple yellow-white Candida lesions. Multiple 1- to 2-cm yellow-white nodules is a typical gross appearance of hepatic candidiasis.
Hepatic *Candida* Abscess H&E section shows a stellate Candida abscess with central necrosis and peripheral fibrosis in a liver wedge biopsy.
Necrosis but Minimal Associated Inflammation This liver specimen shows a large cluster of Candida with associated necrosis, but minimal associated inflammation, in a severely immunocompromised patient. (Courtesy D. Milner, MD.)
*Candida* Morphology This GMS stain shows the mixture of budding yeast, pseudohyphae, and occasional true hyphae that is typical of Candida albicans.
TERMINOLOGY
Definitions
• Infection of liver by Candida fungus
Most common disseminated fungal infection in immunocompromised hosts
Liver involvement is common in disseminated infection
– Rare in immunocompetent patients
ETIOLOGY/PATHOGENESIS
Infectious Agents
• Candida species
Candida albicans most common
Only gold members can continue reading. Log In or Register to continue