Chapter 14
Cancer in Children

Cancer in children is rare, but it is still the leading cause of death from disease in this patient population. The 5-year survival rates in children with cancer have improved from 59% in the 1970s to 83% today.1 Some of the factors leading to improved cure rates in children with cancer include the use of combination chemotherapy, the utilization of immunotherapy, and the participation of many subjects in clinical trials.
Incidence and Types of Cancer
In 2012, approximately 12,060 children (from birth to 14 years of age) in the United States will be diagnosed with cancer, and approximately 1340 will die from the disease, one third of these from leukemia.1
The types of malignancies in children are vastly different from those that affect adults. The most common types of cancer among adults include prostate, breast, lung, and colon. Children (birth to 14 years of age) with leukemias and brain tumors account for 61% of childhood cancers; neuroblastoma and soft tissue or bone sarcomas are less common. Although many adult cancers have associated lifestyle factors that could theoretically be avoided, such as smoking and lifetime exposure to sun, very few environmental factors have been linked to pediatric malignancies. Yet more data are emerging that the developing child may be affected by parental exposures before conception, exposures in utero, and the contents of breast milk.2,3
The incidence of cancer among adolescents and young adults represents only 2% of all invasive cancers. However, the malignancy rate in this age group (15- to 39-year-olds) is three times higher than that in children younger than 15 years. Each year about 70,000 adolescents and young adults will be diagnosed with cancer. The following are the most common cancers diagnosed among the 15- to 39-year-old population in the United States3 (these cancers are discussed in the appropriate chapters):
Leukemia is the most common malignancy in children and the most common type of leukemia is acute lymphoblastic leukemia (ALL), which represents approximately 75% of all pediatric leukemia cases. Although the presenting signs of the various types of leukemia may be similar, the treatment and response to treatment of childhood leukemias vary greatly (see Chapter 30).
CNS tumors are the most common types of solid tumors in children and account for 27% of all childhood cancers1 (see Chapter 20). Not all brain tumors are diagnosed malignant by histologic studies, but even a benign tumor can have devastating effects, depending on the anatomic location. The treatment for brain tumors in children often presents difficulties because therapies, such as radiation, may have debilitating effects on the developing brain, particularly in children younger than 3 years of age.
Lymphoma, including non-Hodgkin lymphoma and Hodgkin lymphoma, is a malignancy that occurs in children and adults. However, the subtypes of lymphoma and treatments in the two populations often differ (see Chapter 30).
Etiology
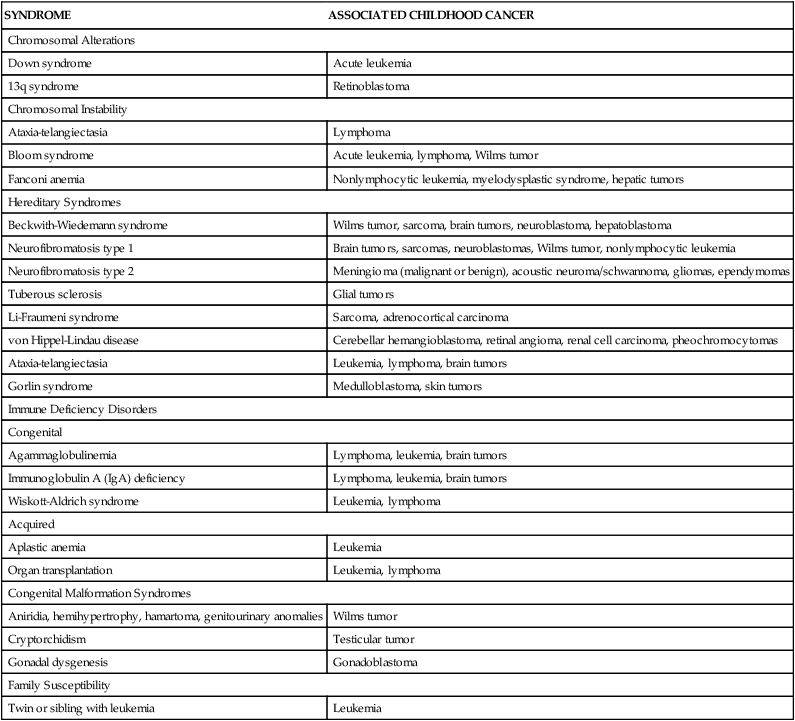
The causes of cancer in children are largely unknown. A few environmental factors are known to predispose a child to cancer, but causal factors have not been established for most childhood cancers. A number of host factors, many of which are genetic risk factors or congenital conditions, have been implicated in the development of childhood cancer (Table 14-1). It is most likely the interaction of many factors that produces cancer, a concept referred to as multiple causation or multifactorial etiology. According to this premise, cancer develops because of the predisposing characteristics of the person and the interaction with environmental causes.
TABLE 14-1
CONGENITAL FACTORS ASSOCIATED WITH CHILDHOOD CANCER
| SYNDROME | ASSOCIATED CHILDHOOD CANCER |
| Chromosomal Alterations | |
| Down syndrome | Acute leukemia |
| 13q syndrome | Retinoblastoma |
| Chromosomal Instability | |
| Ataxia-telangiectasia | Lymphoma |
| Bloom syndrome | Acute leukemia, lymphoma, Wilms tumor |
| Fanconi anemia | Nonlymphocytic leukemia, myelodysplastic syndrome, hepatic tumors |
| Hereditary Syndromes | |
| Beckwith-Wiedemann syndrome | Wilms tumor, sarcoma, brain tumors, neuroblastoma, hepatoblastoma |
| Neurofibromatosis type 1 | Brain tumors, sarcomas, neuroblastomas, Wilms tumor, nonlymphocytic leukemia |
| Neurofibromatosis type 2 | Meningioma (malignant or benign), acoustic neuroma/schwannoma, gliomas, ependymomas |
| Tuberous sclerosis | Glial tumors |
| Li-Fraumeni syndrome | Sarcoma, adrenocortical carcinoma |
| von Hippel-Lindau disease | Cerebellar hemangioblastoma, retinal angioma, renal cell carcinoma, pheochromocytomas |
| Ataxia-telangiectasia | Leukemia, lymphoma, brain tumors |
| Gorlin syndrome | Medulloblastoma, skin tumors |
| Immune Deficiency Disorders | |
| Congenital | |
| Agammaglobulinemia | Lymphoma, leukemia, brain tumors |
| Immunoglobulin A (IgA) deficiency | Lymphoma, leukemia, brain tumors |
| Wiskott-Aldrich syndrome | Leukemia, lymphoma |
| Acquired | |
| Aplastic anemia | Leukemia |
| Organ transplantation | Leukemia, lymphoma |
| Congenital Malformation Syndromes | |
| Aniridia, hemihypertrophy, hamartoma, genitourinary anomalies | Wilms tumor |
| Cryptorchidism | Testicular tumor |
| Gonadal dysgenesis | Gonadoblastoma |
| Family Susceptibility | |
| Twin or sibling with leukemia | Leukemia |
Genetic Factors
Oncogenes and tumor-suppressor genes are associated with the development of childhood cancer (Table 14-2; also see Chapter 12). Proto-oncogenes code for proteins that help to regulate normal cell growth and differentiation. If mutated, proto-oncogenes become oncogenes that help to turn normal cells into cancer cells. Changes produced by specific oncogenes cause the cell cycle to become dysregulated. An example of an oncogene identified in pediatric cancer is N–myc, which is involved in neuroblastoma and glioblastoma. Tumor-suppressor genes arise from genes that normally suppress cancer cell proliferation but have lost their suppressor function, thus leading to uncontrolled growth. Some childhood cancers identified with tumor-suppressor genes include osteosarcoma, leukemia, rhabdomyosarcoma, retinoblastoma, and Wilms tumor.4
TABLE 14-2
SELECTED ONCOGENES AND TUMOR-SUPPRESSOR GENES ASSOCIATED WITH CHILDHOOD CANCER
| GENE | ASSOCIATED PEDIATRIC TUMOR |
| Oncogenes | |
| bcr-abl | Acute lymphoblastic leukemia |
| N-myc | Neuroblastoma |
| c-myb | Neural tumors, leukemia, lymphoma, rhabdomyosarcoma, Wilms tumor, neuroblastoma |
| erb B | Glioblastomas |
| N-ras | Neuroblastoma, leukemia |
| H/K-ras | Neuroblastoma, rhabdomyosarcoma, leukemia |
| ATM | Lymphoma, leukemia |
| Tumor-Suppressor Genes | |
| Rb1 | Retinoblastoma, sarcoma |
| WT1, WT2 | Wilms tumor, leukemia |
| WTC | Wilms tumor |
| NF-1 | Sarcoma, primitive neuroectodermal tumor, juvenile chronic myelocytic leukemia |
| NF-2 | Brain tumors, melanoma, meningiomas |
| p16 | Brain tumors, leukemia |
| TP53 | Sarcoma, leukemia, brain tumors, lymphoma |
| DCC | Ewing sarcoma, rhabdomyosarcoma |
| p16INK4a | Glioma, leukemia |
| p15ARF | Glioblastoma, T-cell ALL |
| CDC2L1 | Non-Hodgkin lymphoma, neuroblastoma |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


