Burkitt Lymphoma
Carlos E. Bueso-Ramos, MD, PhD
Key Facts
Clinical Issues
Median age in adult group is 30 years
In the West, BL presents as abdominal mass
BL may also present as acute leukemia
There are 3 clinical variants of BL
Endemic BL occurs in equatorial Africa and is associated with EBV in almost all cases
Sporadic BL occurs in the West in immunocompetent patients
AIDS-associated BL in patients infected with HIV
Microscopic Pathology
Monomorphic proliferation of medium-sized transformed B cells
Round nuclei, clumped chromatin, basophilic, vacuolated cytoplasm
Multiple nucleoli
Numerous mitoses, macrophages with phagocytosed debris (“starry sky”) Ancillary Tests
BL have germinal center phenotype
IgM(+), CD10(+), Bcl-6(+)
TdT(-), Bcl-2(-)
MYC translocation is characteristic of BL but can be seen in other non-Hodgkin lymphomas
BL karyotype is usually simple, unlike other highgrade lymphomas
Gene expression profiling
Expressed at high levels: MYC and target genes
Expressed at low levels: NF-κB target genes and major histocompatibility complex class I genes
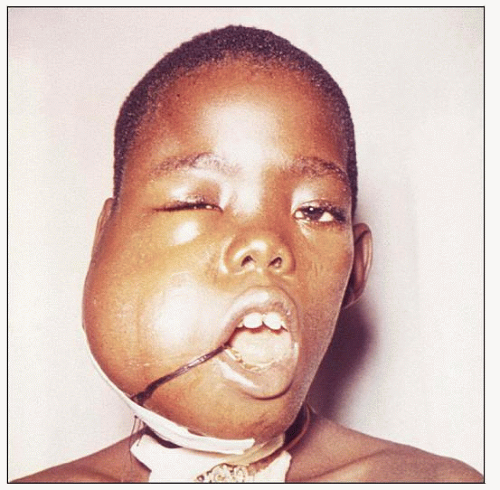 Clinical photograph shows a large tumor of the mandible in an African boy. (Courtesy R. Craig, CDC.) |
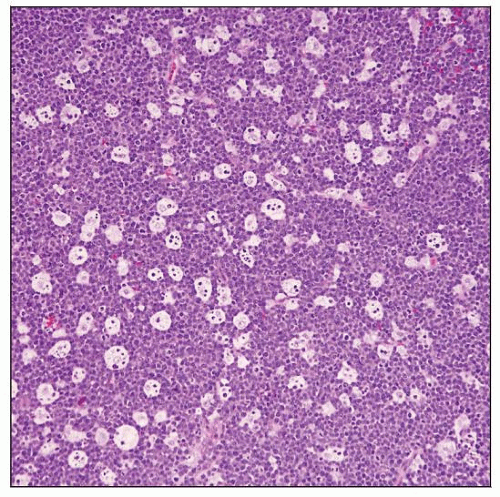 Burkitt Lymphoma. Low-power magnification shows sheets of uniform lymphoma cells with evenly interspersed, reactive, tingible-body macrophages imparting a characteristic “starry sky” pattern. |
TERMINOLOGY
Abbreviations
Burkitt lymphoma (BL) Synonyms
Small noncleaved cell lymphoma, Burkitt type (Working Formulation)
Undifferentiated, Burkitt’s type (Rappaport classification)
Acute lymphoblastic leukemia, L3 type (French-American-British classification)
Definitions
BL is highly aggressive lymphoma that has very short doubling time (˜ 25 hours)
World Health Organization (WHO) states that there is no “gold standard” for diagnosis
Features considered typical of BL
Extranodal sites of involvement
Monomorphic, intermediate-sized cells with basophilic cytoplasm and numerous mitoses
Chromosomal translocations involving MYC
There are 3 clinicopathologic variants of BL
Endemic
Sporadic
Immunodeficiency-associated
ETIOLOGY/PATHOGENESIS
Infectious Agents
There is evidence that BL is a polymicrobial disease
This is particularly true for endemic BL
Association of BL with Epstein-Barr virus (EBV) infection
EBV(+) in
> 95% of cases of endemic BL
˜ 30-40% of immunodeficiency-associated BL
˜ 10-20% of cases of sporadic BL
Endemic BL is associated with Plasmodium falciparum infection
Geographic distribution of endemic BL corresponds to distribution of malaria
Impact on immunity and viral persistence leading to reactivation of latently infected memory B cells
Endemic BL may be associated with infection by arboviruses
Mosquitoes carry arboviruses as they carry malaria
Arboviruses are RNA viruses, and some have oncogenic properties
Chronic antigenic stimulation may exhaust EBVspecific cytotoxic T cells
Impairment of immunosurveillance &/or antigenpresenting function
May thereby allow EBV-driven lymphomagenesis
In endemic BL, malaria or arboviruses provide chronic antigenic stimulation
In immunodeficiency-associated BL, immunosurveillance is impaired by other mechanisms
Human immunodeficiency virus (HIV) is most common
Dietary Factors
Diet may be relevant to endemic BL
In Africa, link to ingestion of plant, Euphorbia tirucalli
Plant has phorbol ester-like substance that may act as tumor promoter
MYC Proto-oncogene
Translocations juxtapose intact MYC gene with enhancer elements of Ig genes, resulting in MYC upregulation
MYC is involved in many cell pathways: Proliferation, transcription, apoptosis
CLINICAL ISSUES
Epidemiology
Incidence
Endemic BL
Common in equatorial Africa, northern South America, Papua New Guinea
Most common type of lymphoma in equatorial Africa
Sporadic BL
˜ 1-2% of lymphomas in industrialized nations
Age
Endemic BL
Children > 2 years of age and adolescents
Median age = 8 years
Sporadic BL
Children and young adults; median age = 30 years
˜ 30-50% of childhood lymphomas in USA
Immunodeficiency-associated BL
Age corresponds to cause of immunodeficiency
Most patients are HIV(+)
Gender
Male:female ratio = 2:5 to 1
Site
Most patients with BL present with extranodal disease
Endemic BL
Jaws and other facial bones are involved in ˜ 50% of patients
Viscera, gonads, gastrointestinal tract
Central nervous system involved in up to 20% of patients
Sporadic BL
Abdomen, particularly the gastrointestinal tract
Lymph nodes are involved in subset of patients
± bone marrow, central nervous system (CNS), or paraspinal mass
Facial bones rarely involved
Small subset of cases can present in leukemic phase
Bone marrow usually extensively involved in these patients
Immunodeficiency-associated BL
Lymph nodes are commonly involved
Bone marrow commonly involved in HIV(+) BL
Presentation
Patients present with rapidly growing mass
B-type symptoms are common Laboratory Tests
Indirect indicators of tumor burden and proliferation
High serum B2-microglobin level
High serum lactate dehydrogenase level
Hyperuricemia can occur due to high tumor cell turnover
Natural History
In absence of therapy, prognosis of BL patients is poor
Rapidly growing progressive disease; often CNS involvement Treatment
Drugs
Approach is rapid administration of multiple chemotherapeutic agents with prophylaxis to CNS &/or testes
Prevent emergence of chemoresistance
Eliminate disease in privileged or sanctuary sites
BL is very sensitive to chemotherapy
Rapid release of intracellular contents following cell death can result in tumor lysis syndrome
Prognosis
With highly intensive therapy, most patients with BL have complete response
Overall survival rate
˜ 80-90% for localized disease
˜ 60-80% for advanced-stage disease
IMAGE FINDINGS
CT Findings
F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT)
All untreated BL are highly FDG avid
Extranodal involvement is identified in > 50% of BL patients
Most patients with sporadic BL have disease localized to abdomen and pelvis
MACROSCOPIC FEATURES
Gross Pathology
Resection specimens of BL often show large extranodal mass, often in abdomen
Fleshy cut surface with areas of necrosis and hemorrhage
MICROSCOPIC PATHOLOGY
Histologic Features
Histologic features of endemic, sporadic, and immunodeficiency-associated BL are identical
Diffuse growth pattern
“Starry sky” pattern is prominent due to presence of numerous tingible-body macrophages with phagocytosed debris
Extremely high mitotic rate
Numerous apoptotic cells and often large areas of necrosis
In subset of cases, BL can be associated with numerous sarcoid-like granulomas



