Chapter 20 Bones and Joints
1 What are the main anatomic portions of tubular long bones?
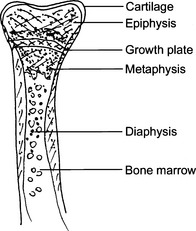
The midportion of a tubular long bone is called the diaphysis. The articular portion of these bones is called epiphysis. The part of the bone between the epiphysis and the diaphysis is called the metaphysis. In growing bones of children and adolescents, the midportion of the metaphysis contains the physis or the cartilaginous growth plate. The calcifying growth plates, easily recognizable on x-ray, are called secondary ossification centers, in contrast to primary ossification centers, a term used for the subperiosteal cortical bone formation. See Fig. 20-1.
2 Name the main bone-forming cells in the bone
 Osteocytes: These mature resting cells are involved in the maintenance of the basic functional and anatomic units of the bone, called osteons. Osteocytes also participate in the maintenance of the blood concentration of calcium and phosphates.
Osteocytes: These mature resting cells are involved in the maintenance of the basic functional and anatomic units of the bone, called osteons. Osteocytes also participate in the maintenance of the blood concentration of calcium and phosphates.

4 What are the most important bone diseases?





DEVELOPMENTAL ABNORMALITIES
6 What is amelia?
A congenital abnormality characterized by an absence of upper or lower extremities or both.
13 List the causes of dwarfism
 Defects in bone formation, such as achondroplasia and osteogenesis imperfecta, and various mucopolysaccharidoses
Defects in bone formation, such as achondroplasia and osteogenesis imperfecta, and various mucopolysaccharidoses


METABOLIC DISORDERS













19 Is primary osteoporosis a single entity?
 Type 1 primary osteoporosis typically occurs in postmenopausal women. It is caused by increased activity of osteoclasts, related to decreased levels of estrogen in the circulation. Lack of estrogen is associated with an increased release of cytokines, such as interleukin (IL)-1 and IL-6, which stimulate osteoclasts.
Type 1 primary osteoporosis typically occurs in postmenopausal women. It is caused by increased activity of osteoclasts, related to decreased levels of estrogen in the circulation. Lack of estrogen is associated with an increased release of cytokines, such as interleukin (IL)-1 and IL-6, which stimulate osteoclasts.
22 Does osteoporosis cause biochemical abnormalities that can be detected in the clinical laboratory?
25 What is the cause of osteomalacia?
 Abnormal vitamin D metabolism (e.g., deficiency of vitamin D receptors or deficiency of 1-hydroxylase, an enzyme that transforms the 25(OH)2 vitamin D in the kidneys into the active form 1,25(OH)2 of vitamin D)
Abnormal vitamin D metabolism (e.g., deficiency of vitamin D receptors or deficiency of 1-hydroxylase, an enzyme that transforms the 25(OH)2 vitamin D in the kidneys into the active form 1,25(OH)2 of vitamin D)


30 Are the bone lesions of hyperparathyroidism localized or diffuse?
 Osteitis fibrosa: Fibrous tissue replacing bone trabeculae in numerous bones or the entire skeleton.
Osteitis fibrosa: Fibrous tissue replacing bone trabeculae in numerous bones or the entire skeleton.




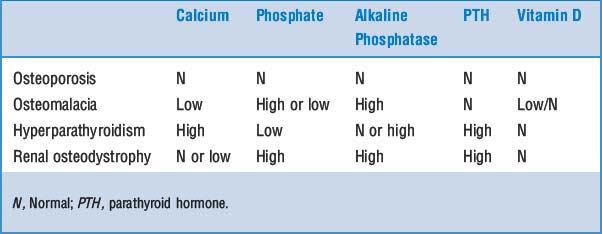
39 Describe how clinical laboratory data help in the diagnosis of metabolic bone diseases
The clinical laboratory has an invaluable role in the study of bone diseases that present radiologically as osteopenia or osteopenia combined with osteosclerosis. The complete workup of the patient will typically require information on the serum calcium, phosphate, and alkaline phosphatase, which then can be supplemented with more expensive tests, such as measurement of PTH and vitamin D in blood. Typical findings are listed in Table 20-1.
FRACTURES





45 How do bone fractures heal?
The healing of bone fractures is a continuous process that can be divided into three stages:
 Provisional callus (procallus): It forms during the first week after fracture and is composed of granulation tissue, newly formed cartilage, and osteoid. It is typically fusiform, filling the defect caused by fracture, but also bulging over the edges of the fractured bone fragments.
Provisional callus (procallus): It forms during the first week after fracture and is composed of granulation tissue, newly formed cartilage, and osteoid. It is typically fusiform, filling the defect caused by fracture, but also bulging over the edges of the fractured bone fragments.








Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


