The osseous portion of the human bone consists of hematopoietic cells, fat cells, and supporting connective tissue separated by irregular bony trabeculae. During bone marrow examination, the marrow particles are aspirated, spread on slides, and a core of bone and marrow (trephine biopsy) is also obtained. The aspirate preparation is valuable for differential cell count and evaluation of cellular morphology; the trephine biopsy is preferred for assessing bone marrow cellularity, determining the number of megakaryocytes, and detecting focal lesions, such as granulomas, lymphoma, or metastatic cancer. Both the aspirate and the biopsy are routinely obtained because of their complementary role in generating the final diagnosis.
BONE MARROW PROCEDURE
Indications and Contraindications
Bone marrow examination is important and effective in the diagnosis of hematological and nonhematological disorders, staging of Hodgkin and non-Hodgkin lymphoma and solid tumors, detection of metastatic malignancy, determination of the extent of bone marrow damage in patients exposed to radiation and drugs, and evaluation of treatment efficacy during chemotherapy and bone marrow transplantation. It is also useful in assessing bone marrow iron store and obtaining microbiology culture in patients with unexplained fever (“fever of unknown origin”), human immunodeficiency virus (HIV) infection, and acquired immunodeficiency syndrome (AIDS). Diagnosis of leukemia and staging of lymphoma are among the most important indications of bone marrow examination (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20). In rare instances, in the absence of peripheral blood abnormality, the diagnosis of leukemia has been made primarily based on bone marrow evaluation (21). Common indications of bone marrow examination are listed in Table 2.1.
The bone marrow examination should be performed only when it is necessary. There are few relative contraindications. Congenital and acquired coagulation factor deficiency and other coagulation abnormalities are considered contraindications by some physicians (22, 23, 24, 25).
Aspiration and Biopsy Sites
The technical steps used in obtaining the bone marrow sample are simple and fairly standardized. An accurate procedure performed by an experienced physician or physician assistant provides optimal material for morphologic evaluation and special studies, and minimizes the need of repeating the biopsy (26, 27, 28, 29).
Although several sites have been used for bone marrow examination, the posterior superior iliac crest (PSIC) remains the preferred site in patients over 1 year of age. In infants in which active hematopoiesis occurs in long bones, aspiration from the anterior medial surface of the tibia is recommended. The tibia is an unsatisfactory site in older individuals because of its variable cellularity and the hardness of the cortical bone. In patients where PSIC is inaccessible, anterior iliac crest can be used. Sternal aspiration is used only when other sites are inaccessible or unsuitable for the procedure, and should not be attempted in infants or children due to its high incidence of associated complications. Furthermore, a trephine biopsy cannot be performed on the sternum because of its anatomy. In esophageal cancer and non-small cell lung cancer, rib segment resection during surgery has been recommended to detect isolated tumor cells in the marrow (30, 31, 32, 33, 34, 35).
Aspiration and Biopsy Techniques
Both aspiration and biopsy are required for bone marrow evaluation and should be performed together. A brief discussion of both procedures is provided here. Before starting, the technique, the complications and alternative diagnostic options are explained to the patient and an informed consent is obtained from the patient or the guardian. The patient should be reassured about the safety of the procedure and, if he or she is overly anxious, a mild sedative may be required. All supplies, including extra syringes, transport media, and’or appropriate anticoagulant tubes for special studies (including flow cytometry, chromosomal analysis, and molecular genetics) should be verified. Supplies for bone marrow procurement are listed in Table 2.2.
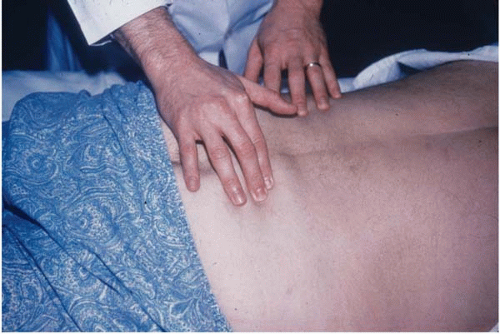
The patient is instructed to lie comfortably on one side (lateral decubitus position) with the knees flexed and the back facing the operator (physician’physician assistant). The PSIC is located lateral to the sacral prominence and is identified by a dimple in the skin forming one of the lateral points of the rhomboid (Fig. 2.1). The skin overlying the iliac crest is marked; the area is sterilized using the standard antiseptic techniques. Bone marrow trays containing necessary sterile items for the procedure are commercially available. Upon opening the tray, all items should be verified to ensure that they are intact and the stylet is working properly. A local anesthetic such as 1% lidocaine is used to anesthetize the overlying skin and, subsequently, the periosteum. Approximately 5 to 10 mL of local anesthetic is usually sufficient. After 5 to 10 minutes, a small skin incision is made with a knife blade. The optimal sequence of performing bone marrow aspiration and biopsy is controversial and depends on the operator’s preference. Procurement of the aspiration prior to trephine biopsy may cause artifactorial hypocellularity and contamination of the core with sinusoidal blood known as “aspiration artifact”; however, this artifact can be avoided if the biopsy is performed in a different angle or from a slightly different site. Tissue trauma of the biopsy prior to aspiration may compromise the quality of subsequent aspiration from the same area due to release of thromboplastic substances.
TABLE 2.1 Indications of Bone Marrow Examination
Diagnosis
Evaluation of Hematologic Disorders
Unexplained anemia, leukopenia, thrombocytopenia, or pancytopenia
Unexplained thrombocytosis, leukocytosis
Acute and chronic leukemia
Myelodysplasic syndromes
Myeloproliferative disorders
Lymphoproliferative disorders
Plasma cell dyscrasia
Staging of Hodgkin disease and non-Hodgkin lymphoma
Aspiration needles, 15 or 16 gauge, different lengths
Biopsy needles, different lengths
Microscope slides, frosted
Disposable plastic syringes
Disposable scalpel
Heparin vacutainers (green-top)
EDTA vacutainers (purple-top)
Zip-lock plastic bags
Small blowing fan
Figure 2.1 Bone marrow examination, locating the posterior superior iliac crest (PSIC).
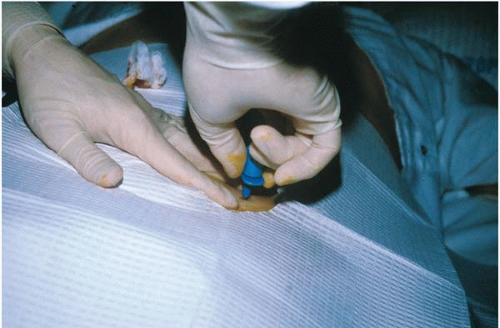
Figure 2.2 Bone marrow examination, placing an Illinois aspiration needle into the marrow.
When performing the aspiration, the needle is pushed through the skin and periosteum with a firm, twisting, clockwise and counterclockwise motion until it penetrates through the cortical bone into the medullary cavity (Fig. 2.2). When the cortical bone is penetrated, the operator usually feels a subtle decrease in resistance. After achieving a firm fixation of the needle shaft in the bone marrow cavity, the central stylet is unlocked and removed immediately. A large, sterile, heparinized syringe is then attached. The patient should be warned that he or she might experience an unpleasant sensation or a significant degree of pain during aspiration. Approximately 1 to 2 mL of bone marrow is quickly aspirated into the syringe (Fig. 2.3). The initial aspirate should be used for morphologic evaluation; additional aspirate can be obtained for special studies, including flow cytometry, chromosomal analysis, molecular genetics, and microbiology culturing.
After the bone marrow aspirate is obtained, the biopsy needle is advanced in a slightly different angle for 1 to 2 cm (Fig. 2.4). The needle is rotated in a circular, back-and-forth motion several times to dislodge the core from its surrounding tissue, and the needle is gently withdrawn. The core biopsy is dislodged from the needle by inserting another stylet or probe through the needle (Fig. 2.5). When the procedure is finished, the biopsy site is placed under pressure for 5 minutes (10 to 15 minutes in patients with thrombocytopenia) before being covered by a small bandage (26, 27, 28, 29). The biopsy specimens should be labeled and processed separately (36,37).
Only gold members can continue reading. Log In or Register to continue