Patient Story
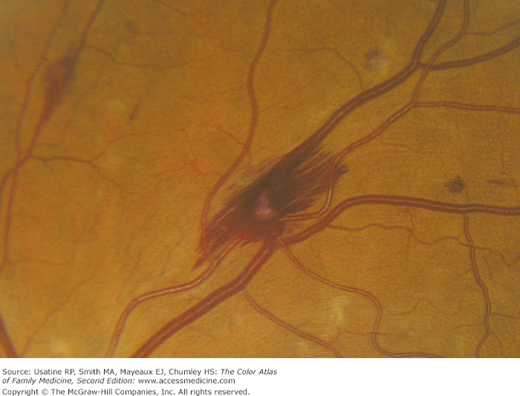
A 25-year-old man presented to the office because he had been feeling tired and feverish for several weeks. He admitted to injecting heroin regularly in the last 2 months. On examination, he was febrile and had a heart murmur of which he was previously unaware. His fingernails showed splinter hemorrhages (Figure 50-1). His funduscopic examination revealed Roth spots (Figures 50-2 and 50-3). An echocardiogram demonstrated vegetation on the tricuspid valve. He was hospitalized and treated empirically for bacterial endocarditis. After his blood cultures returned Staphylococcus aureus, his regimen was adjusted based on sensitivities and continued for 6 weeks.


Introduction
Bacterial endocarditis is a serious infection seen most commonly in patients with prosthetic valves; injection drug users; patients with HIV, especially those who use intravenous (IV) drugs; and patients who are immunosuppressed. Diagnosis is made based on Duke Criteria. Treatment is IV antibiotics. Mortality, despite treatment, is 26% to 37%.
Epidemiology
- 5.0 to 7.9 cases per 100,000 patient-years.1
- Historically more common in men; however, the incidence in women is increasing. Men and women 8.6 to 12.7 and 1.4 to 6.7 cases per 100,000 person-years, respectively.1
- Average age has increased from 46.5 years (1980-1984) to 70 years (2001-2006).1
- Incidence in IV drug users is 3 per 1000 person-years or 1% to 5% per year.2
- Incidence in HIV-positive IV drug users is 13.8 per 1000 person-years.2
- Historically more common in men; however, the incidence in women is increasing. Men and women 8.6 to 12.7 and 1.4 to 6.7 cases per 100,000 person-years, respectively.1
- Seen in immunosuppressed patients with central venous catheters or hemodialysis patients.
- Fifty percent healthcare-associated, 43% community-acquired, and 7.5% nosocomial.1
- Mortality ranges from 16% to 37%.3
- Fifty percent healthcare-associated, 43% community-acquired, and 7.5% nosocomial.1
- Prosthetic valve endocarditis makes up 10% to 15% of endocarditis cases.4
- Incidence of 0.1% to 2.3% person-year.4
- Can occur early (2 months after surgery) or late.
- Incidence of 0.1% to 2.3% person-year.4
Etiology and Pathophysiology
- Endothelium is injured by mechanical or inflammatory processes.
- Microbes adhere to compromised endothelium during transient bacteremia.
- Common organisms include S. aureus (IV drug users, nosocomial infections, prosthetic valve patients), Streptococcus bovis (elderly patients), enterococci (nosocomial infections), and Staphylococcus epidermis (early infection in prosthetic valve patients).
- Blood contacts subendothelial factors, which promotes coagulation.
- Pathogens bind and activate monocyte, cytokine, and tissue factor production, enlarging the vegetations on the heart valves.
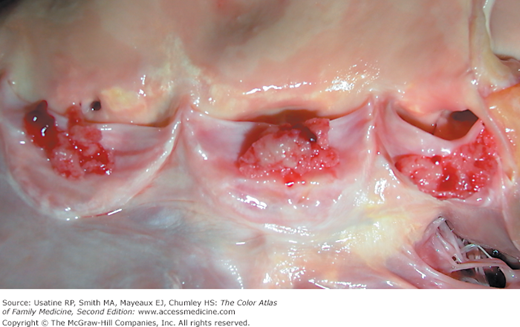
- The vegetations enlarge and damage the heart valves (Figure 50-4). This process can lead to death if not treated adequately in time.
- Septic emboli can occur, most commonly in the brain, spleen, or kidney.4
Diagnosis
- Duke criteria use a combination of history, physical examination, laboratory, and echocardiogram findings, and have a sensitivity of approximately 80% across several studies.5
- Diagnosis is considered definite when patients have two major, one major and three minor, or five minor criteria.5
- Diagnosis is considered possible with one major and one minor or three minor criteria.5
- Major criteria include:5
- Two separate blood cultures positive with:
- Streptococcus viridans, S. bovis, Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella.
- Community-acquired S. aureus or Enterococcus without a primary focus.
- Microorganisms consistent with prior positive blood cultures in infective endocarditis.
- Streptococcus viridans, S. bovis, Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella.
- Endocardial involvement as evidenced by:
- Echocardiogram evidence of vegetation, abscess, or new partial dehiscence of a prosthetic valve.
- New valvular regurgitation.
- Echocardiogram evidence of vegetation, abscess, or new partial dehiscence of a prosthetic valve.
- Minor criteria include:5
- Predisposition (e.g., heart condition such as a congenital or acquired valvular defect, injection drug use, prior history of endocarditis).
- Temperature >38°C (100.4°F).
- Clinical signs: arterial emboli, septic pulmonary infarcts, mycotic aneurysms, intracranial hemorrhages, Janeway lesions (Figures 50-5 and 50-6).
- Glomerulonephritis, Osler nodes, Roth spots, or positive rheumatoid factor (Figures 50-2, 50-3, and 50-6

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


- Predisposition (e.g., heart condition such as a congenital or acquired valvular defect, injection drug use, prior history of endocarditis).
- Two separate blood cultures positive with:
