Atypical presentation and pain patterns are common, especially in the very old or the very young. Diagnosing appendicitis in children can be especially challenging because they tend to respond so dramatically to stimulation and obtaining an accurate history may be difficult. In addition, it is important to remember that the smaller omentum found in children may be less likely to wall off an appendiceal perforation. Observing the child in a quiet surrounding may be helpful.
Signs and symptoms of appendicitis can be subtle in the elderly who may not react as vigorously to appendicitis as younger people. Pain, if noticed, may be minimal and have originated in the right lower quadrant or, otherwise, where the appendix is located. It may never have been noticed to be intermittent, or there may only be significant discomfort with deep palpation. Nausea, anorexia, and emesis may be the predominant complaints. The rare patient may even present with signs and symptoms of distal bowel obstruction secondary to appendiceal inflammation and phlegmon or abscess formation.
LABORATORY TESTING
Laboratory testing does not identify patients with appendicitis but can help the clinician work through the differential diagnosis. The white blood cell count is only mildly to moderately elevated in approximately 70% of patients with simple appendicitis (with a leukocytosis of 10,000–18,000 cells/μL). A “left shift” toward immature polymorphonuclear leukocytes is present in >95% of cases. A sickle cell preparation may be prudent to obtain in those of African, Spanish, Mediterranean, or Indian ancestry. Serum amylase and lipase levels should be measured.
Urinalysis is indicated to help exclude genitourinary conditions that may mimic acute appendicitis, but a few red or white blood cells may be present as a nonspecific finding. However, an inflamed appendix that abuts the ureter or bladder may cause sterile pyuria or hematuria. Every woman of childbearing age should have a pregnancy test. Cervical cultures are indicated if pelvic inflammatory disease is suspected. Anemia and guaiac-positive stools should raise concern about the presence of other diseases or complications such as cancer.
IMAGING
Plain films of the abdomen are rarely helpful and so are not routinely obtained unless the clinician is worried about other conditions such as intestinal obstruction, perforated viscus, or ureterolithiasis. Less than 5% of patients will present with an opaque fecalith in the right lower quadrant. The presence of a fecalith is not diagnostic of appendicitis, although its presence in an appropriate location where the patient complains of pain is suggestive.
The effectiveness of ultrasonography as a tool to diagnosis appendicitis is highly operator dependent. Even in very skilled hands, the appendix may not be visualized. Its overall sensitivity is 0.86, with a specificity of 0.81. Ultrasonography, especially intravaginal techniques, appears to be most useful for identifying pelvic pathology in women. Ultrasonographic findings suggesting the presence of appendicitis include wall thickening, an increased appendiceal diameter, and the presence of free fluid.
The sensitivity and specificity of computed tomography (CT) are 0.94 and 0.95, respectively. Thus, CT imaging, given its high negative predictive value, may be helpful if the diagnosis is in doubt, although studies performed early in the course of disease may not have any typical radiographic findings. Suggestive findings on CT examination include dilatation >6 mm with wall thickening, a lumen that does not fill with enteric contrast, and fatty tissue stranding or air surrounding the appendix, which suggests inflammation (Figs. 356-3 and 356-4). The presence of luminal air or contrast is not consistent with a diagnosis of appendicitis. Furthermore, nonvisualization of the appendix is a nonspecific finding that should not be used to rule out the presence of appendiceal or periappendiceal inflammation.
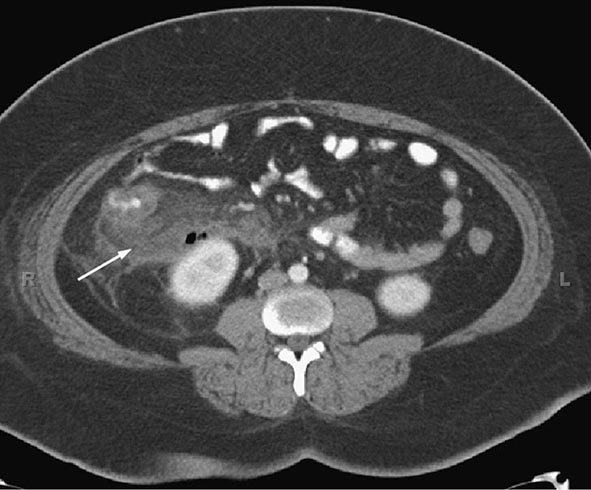
FIGURE 356-3 Computed tomography with oral and intravenous contrast of acute appendicitis. There is thickening of the wall of the appendix and periappendiceal stranding (arrow).
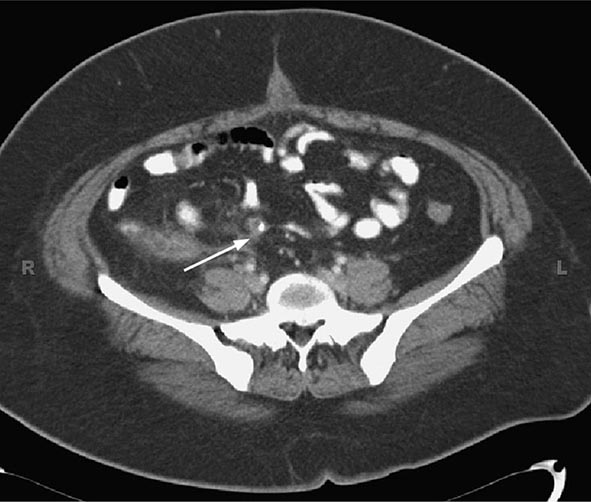
FIGURE 356-4 Appendiceal fecalith (arrow).
SPECIAL PATIENT POPULATIONS
Appendicitis in the most common extrauterine general surgical emergency observed during pregnancy. Early symptoms of appendicitis such as nausea and anorexia may be overlooked. Diagnosing appendicitis in pregnant patients may be especially difficult because as the uterus enlarges the appendix may be pushed higher along the right flank even to the right upper quadrant or because the gravid uterus may obscure typical physical findings. Ultrasonography may facilitate early diagnosis. A high index of suspicion is required because of the effects of unrecognized and untreated appendicitis on the fetus. For example, the fetal mortality rate is four times greater (from 5 to 20%) in patients with perforation.
Immunocompromised patients may present with only mild tenderness and may have many other disease processes in their differential diagnosis, including atypical infections from mycobacteria, Cytomegalovirus, or other fungi. Enterocolitis is a concern and may be present in patients who present with abdominal pain, fever, and neutropenia due to chemotherapy. CT imaging may be very helpful, although it is important not to be overly cautious and delay operative intervention for those patients who are believed to have appendicitis.
ACUTE PERITONITIS
Acute peritonitis, or inflammation of the visceral and parietal peritoneum, is most often but not always infectious in origin, resulting from perforation of a hollow viscus. This is called secondary peritonitis, as opposed to primary or spontaneous peritonitis, when a specific intraabdominal source cannot be identified. In either instance, the inflammation can be localized or diffuse.
ETIOLOGY
Infective organisms may contaminate the peritoneal cavity after spillage from a hollow viscus, because of a penetrating wound of the abdominal wall, or because of the introduction of a foreign object like a peritoneal dialysis catheter or port that becomes infected. Secondary peritonitis most commonly results from perforation of the appendix, colonic diverticuli, or the stomach and duodenum. It may also occur as a complication of bowel infarction or incarceration, cancer, inflammatory bowel disease, and intestinal obstruction or volvulus. Conditions that may cause secondary bacterial peritonitis and their mechanisms are listed in Table 356-5. Over 90% of the cases of primary or spontaneous bacterial peritonitis occur in patients with ascites or hypoproteinemia (<1 g/L).
CONDITIONS LEADING TO SECONDARY BACTERIAL PERITONITIS |
Aseptic peritonitis is most commonly caused by the abnormal presence of physiologic fluids like gastric juice, bile, pancreatic enzymes, blood, or urine. It can also be caused by the effects of normally sterile foreign bodies like surgical sponges or instruments. More rarely, it occurs as a complication of systemic diseases like lupus erythematosus, porphyria, and familial Mediterranean fever. The chemical irritation caused by stomach acid and activated pancreatic enzymes is extreme and secondary bacterial infection may occur.
CLINICAL FEATURES
The cardinal signs and symptoms of peritonitis are acute, typically severe, abdominal pain with tenderness and fever. How the patient’s complaints of pain are manifested depends on their overall physical health and whether the inflammation is diffuse or localized. Elderly and immunosuppressed patients may not respond as aggressively to the irritation. Diffuse, generalized peritonitis is most often recognized as diffuse abdominal tenderness with local guarding, rigidity, and other evidence of parietal peritoneal irritation. Physical findings may only be identified in a specific region of the abdomen if the intraperitoneal inflammatory process is limited or otherwise contained as may occur in patients with uncomplicated appendicitis or diverticulitis. Bowel sounds are usually absent to hypoactive.
Most patients present with tachycardia and signs of volume depletion with hypotension. Laboratory testing typically reveals a significant leukocytosis, and patients may be severely acidotic. Radiographic studies may show dilatation of the bowel and associated bowel wall edema. Free air, or other evidence of leakage, requires attention and could represent a surgical emergency. In stable patients in whom ascites is present, diagnostic paracentesis is indicated, where the fluid is tested for protein and lactate dehydrogenase and the cell count is measured.
THERAPY AND PROGNOSIS
Whereas mortality rates can be less than 10% for reasonably healthy patients with relatively uncomplicated, localized peritonitis, mortality rates >40% have been reported for the elderly or immunocompromised. Successful treatment depends on correcting any electrolyte abnormalities, restoration of fluid volume and stabilization of the cardiovascular system, appropriate antibiotic therapy, and surgical correction of any underlying abnormalities.
ACKNOWLEDGMENT
The wisdom and expertise of Dr. William Silen is gratefully acknowledged in this updated chapter on acute appendicitis and peritonitis.
SECTION 2 | LIVER AND BILIARY TRACT DISEASE |
357 | Approach to the Patient with Liver Disease |
A diagnosis of liver disease usually can be made accurately by careful elicitation of the patient’s history, physical examination, and application of a few laboratory tests. In some circumstances, radiologic examinations are helpful or, indeed, diagnostic. Liver biopsy is considered the criterion standard in evaluation of liver disease but is now needed less for diagnosis than for grading and staging of disease. This chapter provides an introduction to diagnosis and management of liver disease, briefly reviewing the structure and function of the liver; the major clinical manifestations of liver disease; and the use of clinical history, physical examination, laboratory tests, imaging studies, and liver biopsy.
LIVER STRUCTURE AND FUNCTION
The liver is the largest organ of the body, weighing 1–1.5 kg and representing 1.5–2.5% of the lean body mass. The size and shape of the liver vary and generally match the general body shape—long and lean or squat and square. This organ is located in the right upper quadrant of the abdomen under the right lower rib cage against the diaphragm and projects for a variable extent into the left upper quadrant. It is held in place by ligamentous attachments to the diaphragm, peritoneum, great vessels, and upper gastrointestinal organs. The liver receives a dual blood supply; ~20% of the blood flow is oxygen-rich blood from the hepatic artery, and 80% is nutrient-rich blood from the portal vein arising from the stomach, intestines, pancreas, and spleen.
The majority of cells in the liver are hepatocytes, which constitute two-thirds of the organ’s mass. The remaining cell types are Kupffer cells (members of the reticuloendothelial system), stellate (Ito or fat-storing) cells, endothelial and blood vessel cells, bile ductular cells, and cells of supporting structures. Viewed by light microscopy, the liver appears to be organized in lobules, with portal areas at the periphery and central veins in the center of each lobule. However, from a functional point of view, the liver is organized into acini, with both hepatic arterial and portal venous blood entering the acinus from the portal areas (zone 1) and then flowing through the sinusoids to the terminal hepatic veins (zone 3); the intervening hepatocytes constitute zone 2. The advantage of viewing the acinus as the physiologic unit of the liver is that this perspective helps to explain the morphologic patterns and zonality of many vascular and biliary diseases not explained by the lobular arrangement.
Portal areas of the liver consist of small veins, arteries, bile ducts, and lymphatics organized in a loose stroma of supporting matrix and small amounts of collagen. Blood flowing into the portal areas is distributed through the sinusoids, passing from zone 1 to zone 3 of the acinus and draining into the terminal hepatic veins (“central veins”). Secreted bile flows in the opposite direction—i.e., in a counter-current pattern from zone 3 to zone 1. The sinusoids are lined by unique endothelial cells that have prominent fenestrae of variable sizes, allowing the free flow of plasma but not of cellular elements. The plasma is thus in direct contact with hepatocytes in the subendothelial space of Disse.
Hepatocytes have distinct polarity. The basolateral side of the hepatocyte lines the space of Disse and is richly lined with microvilli; it exhibits endocytotic and pinocytotic activity, with passive and active uptake of nutrients, proteins, and other molecules. The apical pole of the hepatocyte forms the canalicular membranes through which bile components are secreted. The canaliculi of hepatocytes form a fine network, which fuses into the bile ductular elements near the portal areas. Kupffer cells usually lie within the sinusoidal vascular space and represent the largest group of fixed macrophages in the body. The stellate cells are located in the space of Disse but are not usually prominent unless activated, when they produce collagen and matrix. Red blood cells stay in the sinusoidal space as blood flows through the lobules, but white blood cells can migrate through or around endothelial cells into the space of Disse and from there to portal areas, where they can return to the circulation through lymphatics.
Hepatocytes perform numerous and vital roles in maintaining homeostasis and health. These functions include the synthesis of most essential serum proteins (albumin, carrier proteins, coagulation factors, many hormonal and growth factors), the production of bile and its carriers (bile acids, cholesterol, lecithin, phospholipids), the regulation of nutrients (glucose, glycogen, lipids, cholesterol, amino acids), and the metabolism and conjugation of lipophilic compounds (bilirubin, anions, cations, drugs) for excretion in the bile or urine. Measurement of these activities to assess liver function is complicated by the multiplicity and variability of these functions. The most commonly used liver “function” tests are measurements of serum bilirubin, serum albumin, and prothrombin time. The serum bilirubin level is a measure of hepatic conjugation and excretion; the serum albumin level and prothrombin time are measures of protein synthesis. Abnormalities of bilirubin, albumin, and prothrombin time are typical of hepatic dysfunction. Frank liver failure is incompatible with life, and the functions of the liver are too complex and diverse to be subserved by a mechanical pump; a dialysis membrane; or a concoction of infused hormones, proteins, and growth factors.
LIVER DISEASES
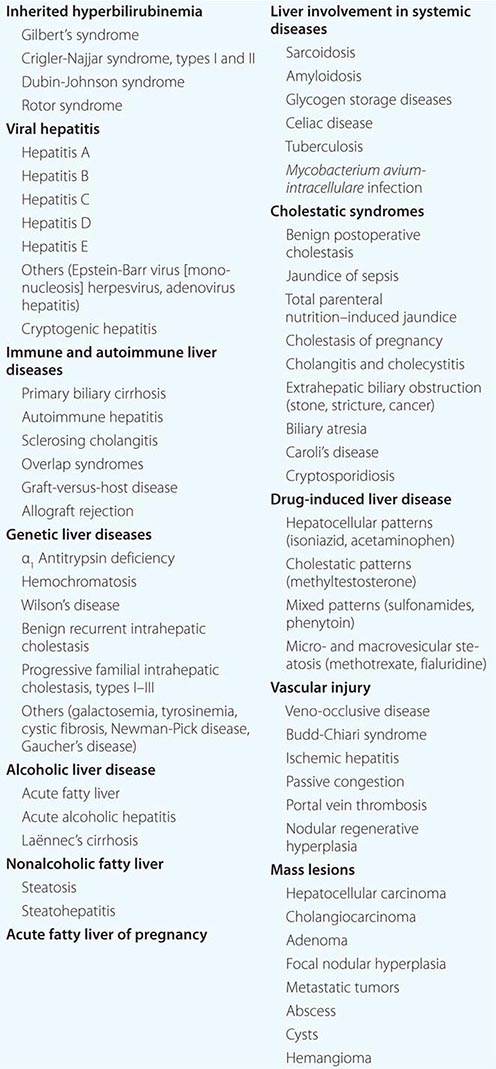
While there are many causes of liver disease (Table 357-1), these disorders generally present clinically in a few distinct patterns and are usually classified as hepatocellular, cholestatic (obstructive), or mixed. In hepatocellular diseases (such as viral hepatitis and alcoholic liver disease), features of liver injury, inflammation, and necrosis predominate. In cholestatic diseases (such as gallstone or malignant obstruction, primary biliary cirrhosis, and some drug-induced liver diseases), features of inhibition of bile flow predominate. In a mixed pattern, features of both hepatocellular and cholestatic injury are present (such as in cholestatic forms of viral hepatitis and many drug-induced liver diseases). The pattern of onset and prominence of symptoms can rapidly suggest a diagnosis, particularly if major risk factors are considered, such as the age and sex of the patient and a history of exposure or risk behaviors.
LIVER DISEASES |
Typical presenting symptoms of liver disease include jaundice, fatigue, itching, right-upper-quadrant pain, nausea, poor appetite, abdominal distention, and intestinal bleeding. At present, however, many patients are diagnosed with liver disease who have no symptoms and who have been found to have abnormalities in biochemical liver tests as a part of a routine physical examination or screening for blood donation or for insurance or employment. The wide availability of batteries of liver tests makes it relatively simple to demonstrate the presence of liver injury as well as to rule it out in someone in whom liver disease is suspected.
Evaluation of patients with liver disease should be directed at (1) establishing the etiologic diagnosis, (2) estimating disease severity (grading), and (3) establishing the disease stage (staging). Diagnosis should focus on the category of disease (hepatocellular, cholestatic, or mixed injury) as well as on the specific etiologic diagnosis. Grading refers to assessment of the severity or activity of disease—active or inactive as well as mild, moderate, or severe. Staging refers to estimation of the point in the course of the natural history of the disease, whether early or late; or precirrhotic, cirrhotic, or end-stage. This chapter introduces general, salient concepts in the evaluation of patients with liver disease that help lead to the diagnoses discussed in subsequent chapters.
CLINICAL HISTORY
The clinical history should focus on the symptoms of liver disease—their nature, patterns of onset, and progression—and on potential risk factors for liver disease. The manifestations of liver disease include constitutional symptoms such as fatigue, weakness, nausea, poor appetite, and malaise and the more liver-specific symptoms of jaundice, dark urine, light stools, itching, abdominal pain, and bloating. Symptoms can also suggest the presence of cirrhosis, end-stage liver disease, or complications of cirrhosis such as portal hypertension. Generally, the constellation of symptoms and their patterns of onset rather than a specific symptom points to an etiology.
Fatigue is the most common and most characteristic symptom of liver disease. It is variously described as lethargy, weakness, listlessness, malaise, increased need for sleep, lack of stamina, and poor energy. The fatigue of liver disease typically arises after activity or exercise and is rarely present or severe after adequate rest; i.e., it is “afternoon” rather than “morning” fatigue. Fatigue in liver disease is often intermittent and variable in severity from hour to hour and day to day. In some patients, it may not be clear whether fatigue is due to the liver disease or to other problems such as stress, anxiety, sleep disturbance, or a concurrent illness.
Nausea occurs with more severe liver disease and may accompany fatigue or be provoked by smelling food odors or eating fatty foods. Vomiting can occur but is rarely persistent or prominent. Poor appetite with weight loss occurs frequently in acute liver disease but is rare in chronic disease except when cirrhosis is present and advanced. Diarrhea is uncommon in liver disease except with severe jaundice, in which a lack of bile acids reaching the intestine can lead to steatorrhea.
Right-upper-quadrant discomfort or ache (“liver pain”) occurs in many liver diseases and is usually marked by tenderness over the liver area. The pain arises from stretching or irritation of Glisson’s capsule, which surrounds the liver and is rich in nerve endings. Severe pain is most typical of gallbladder disease, liver abscess, and severe veno-occlusive disease but is also an occasional accompaniment of acute hepatitis.
Itching occurs with acute liver disease, appearing early in obstructive jaundice (from biliary obstruction or drug-induced cholestasis) and somewhat later in hepatocellular disease (acute hepatitis). Itching also occurs in chronic liver diseases—typically the cholestatic forms such as primary biliary cirrhosis and sclerosing cholangitis, in which it is often the presenting symptom, preceding the onset of jaundice. However, itching can occur in any liver disease, particularly once cirrhosis develops.
Jaundice is the hallmark symptom of liver disease and perhaps the most reliable marker of severity. Patients usually report darkening of the urine before they notice scleral icterus. Jaundice is rarely detectable with a bilirubin level <43 μmol/L (2.5 mg/dL). With severe cholestasis, there will also be lightening of the color of the stools and steatorrhea. Jaundice without dark urine usually indicates indirect (unconjugated) hyperbilirubinemia and is typical of hemolytic anemia and the genetic disorders of bilirubin conjugation, the common and benign form being Gilbert’s syndrome and the rare and severe form being Crigler-Najjar syndrome. Gilbert’s syndrome affects up to 5% of the general population; the jaundice in this condition is more noticeable after fasting and with stress.
Major risk factors for liver disease that should be sought in the clinical history include details of alcohol use, medication use (including herbal compounds, birth control pills, and over-the-counter medications), personal habits, sexual activity, travel, exposure to jaundiced or other high-risk persons, injection drug use, recent surgery, remote or recent transfusion of blood or blood products, occupation, accidental exposure to blood or needlestick, and familial history of liver disease.
For assessing the risk of viral hepatitis, a careful history of sexual activity is of particular importance and should include the number of lifetime sexual partners and, for men, a history of having sex with men. Sexual exposure is a common mode of spread of hepatitis B but is rare for hepatitis C. A family history of hepatitis, liver disease, and liver cancer is also important. Maternal-infant transmission occurs with both hepatitis B and C. Vertical spread of hepatitis B can now be prevented by passive and active immunization of the infant at birth. Vertical spread of hepatitis C is uncommon, but there are no reliable means of prevention. Transmission is more common among HIV-co-infected mothers and is also linked to prolonged and difficult labor and delivery, early rupture of membranes, and internal fetal monitoring. A history of injection drug use, even in the remote past, is of great importance in assessing the risk for hepatitis B and C. Injection drug use is now the single most common risk factor for hepatitis C. Transfusion with blood or blood products is no longer an important risk factor for acute viral hepatitis. However, blood transfusions received before the introduction of sensitive enzyme immunoassays for antibody to hepatitis C virus in 1992 is an important risk factor for chronic hepatitis C. Blood transfusion before 1986, when screening for antibody to hepatitis B core antigen was introduced, is also a risk factor for hepatitis B. Travel to a developing area of the world, exposure to persons with jaundice, and exposure to young children in day-care centers are risk factors for hepatitis A. Tattooing and body piercing (for hepatitis B and C) and eating shellfish (for hepatitis A) are frequently mentioned but are actually types of exposure that quite rarely lead to the acquisition of hepatitis.
![]() Hepatitis E is one of the more common causes of jaundice in Asia and Africa but is uncommon in developed nations. Recently, non-travel-related (autochthonous) cases of hepatitis E have been described in developed countries, including the United States. These cases appear to be due to strains of hepatitis E virus that are endemic in swine and some wild animals (genotypes 3 and 4). While occasional cases are associated with eating raw or undercooked pork or game (deer and wild boars), most cases of hepatitis E occur without known exposure, predominantly in elderly man without typical risk factors for viral hepatitis. Hepatitis E infection can become chronic in immunosuppressed individuals (such as transplant recipients, patients receiving chemotherapy, or patients with HIV infection), in whom it presents with abnormal serum enzymes in the absence of markers of hepatitis B or C.
Hepatitis E is one of the more common causes of jaundice in Asia and Africa but is uncommon in developed nations. Recently, non-travel-related (autochthonous) cases of hepatitis E have been described in developed countries, including the United States. These cases appear to be due to strains of hepatitis E virus that are endemic in swine and some wild animals (genotypes 3 and 4). While occasional cases are associated with eating raw or undercooked pork or game (deer and wild boars), most cases of hepatitis E occur without known exposure, predominantly in elderly man without typical risk factors for viral hepatitis. Hepatitis E infection can become chronic in immunosuppressed individuals (such as transplant recipients, patients receiving chemotherapy, or patients with HIV infection), in whom it presents with abnormal serum enzymes in the absence of markers of hepatitis B or C.
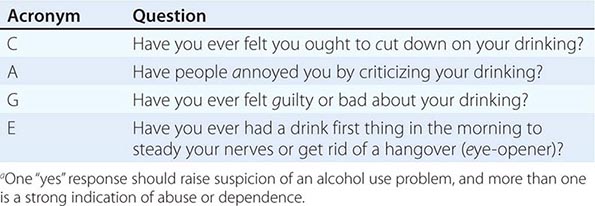
A history of alcohol intake is important in assessing the cause of liver disease and also in planning management and recommendations. In the United States, for example, at least 70% of adults drink alcohol to some degree, but significant alcohol intake is less common; in population-based surveys, only 5% of individuals have more than two drinks per day, the average drink representing 11–15 g of alcohol. Alcohol consumption associated with an increased rate of alcoholic liver disease is probably more than two drinks (22–30 g) per day in women and three drinks (33–45 g) in men. Most patients with alcoholic cirrhosis have a much higher daily intake and have drunk excessively for ≥10 years before onset of liver disease. In assessing alcohol intake, the history should also focus on whether alcohol abuse or dependence is present. Alcoholism is usually defined by the behavioral patterns and consequences of alcohol intake, not by the amount. Abuse is defined by a repetitive pattern of drinking alcohol that has adverse effects on social, family, occupational, or health status. Dependence is defined by alcohol-seeking behavior, despite its adverse effects. Many alcoholics demonstrate both dependence and abuse, and dependence is considered the more serious and advanced form of alcoholism. A clinically helpful approach to diagnosis of alcohol dependence and abuse is the use of the CAGE questionnaire (Table 357-2), which is recommended for all medical history-taking.
CAGE QUESTIONSa |
Family history can be helpful in assessing liver disease. Familial causes of liver disease include Wilson’s disease; hemochromatosis and α1 antitrypsin deficiency; and the more uncommon inherited pediatric liver diseases—i.e., familial intrahepatic cholestasis, benign recurrent intrahepatic cholestasis, and Alagille syndrome. Onset of severe liver disease in childhood or adolescence in conjunction with a family history of liver disease or neuropsychiatric disturbance should lead to investigation for Wilson’s disease. A family history of cirrhosis, diabetes, or endocrine failure and the appearance of liver disease in adulthood suggests hemochromatosis and should prompt investigation of iron status. Abnormal iron studies in adult patients warrant genotyping of the HFE gene for the C282Y and H63D mutations typical of genetic hemochromatosis. In children and adolescents with iron overload, other non-HFE causes of hemochromatosis should be sought. A family history of emphysema should provoke investigation of α1 antitrypsin levels and, if levels are low, for protease inhibitor (Pi) genotype.
PHYSICAL EXAMINATION
The physical examination rarely uncovers evidence of liver dysfunction in a patient without symptoms or laboratory findings, nor are most signs of liver disease specific to one diagnosis. Thus, the physical examination complements rather than replaces the need for other diagnostic approaches. In many patients, the physical examination is normal unless the disease is acute or severe and advanced. Nevertheless, the physical examination is important in that it can yield the first evidence of hepatic failure, portal hypertension, and liver decompensation. In addition, the physical examination can reveal signs—related either to risk factors or to associated diseases or findings—that point to a specific diagnosis.
Typical physical findings in liver disease are icterus, hepatomegaly, hepatic tenderness, splenomegaly, spider angiomata, palmar erythema, and excoriations. Signs of advanced disease include muscle wasting, ascites, edema, dilated abdominal veins, hepatic fetor, asterixis, mental confusion, stupor, and coma. In male patients with cirrhosis, particularly that related to alcohol use, signs of hyperestrogenemia such as gynecomastia, testicular atrophy, and loss of male-pattern hair distribution may be found.
Icterus is best appreciated when the sclera is inspected under natural light. In fair-skinned individuals, a yellow tinge to the skin may be obvious. In dark-skinned individuals, examination of the mucous membranes below the tongue can demonstrate jaundice. Jaundice is rarely detectable if the serum bilirubin level is <43 μmol/L (2.5 mg/dL) but may remain detectable below this level during recovery from jaundice (because of protein and tissue binding of conjugated bilirubin).
Spider angiomata and palmar erythema occur in both acute and chronic liver disease; these manifestations may be especially prominent in persons with cirrhosis but can develop in normal individuals and are frequently found during pregnancy. Spider angiomata are superficial, tortuous arterioles and—unlike simple telangiectases—typically fill from the center outward. Spider angiomata occur only on the arms, face, and upper torso; they can be pulsatile and may be difficult to detect in dark-skinned individuals.
Hepatomegaly is not a highly reliable sign of liver disease because of variability in the liver’s size and shape and the physical impediments to assessment of liver size by percussion and palpation. Marked hepatomegaly is typical of cirrhosis, veno-occlusive disease, infiltrative disorders such as amyloidosis, metastatic or primary cancers of the liver, and alcoholic hepatitis. Careful assessment of the liver edge may also reveal unusual firmness, irregularity of the surface, or frank nodules. Perhaps the most reliable physical finding in the liver examination is hepatic tenderness. Discomfort when the liver is touched or pressed upon should be carefully sought with percussive comparison of the right and left upper quadrants.
Splenomegaly, which occurs in many medical conditions, can be a subtle but significant physical finding in liver disease. The availability of ultrasound methods for assessment of the spleen allows confirmation of the physical finding.
Signs of advanced liver disease include muscle wasting and weight loss as well as hepatomegaly, bruising, ascites, and edema. Ascites is best appreciated by attempts to detect shifting dullness by careful percussion. Ultrasound examination will confirm the finding of ascites in equivocal cases. Peripheral edema can occur with or without ascites. In patients with advanced liver disease, other factors frequently contribute to edema formation, including hypoalbuminemia, venous insufficiency, heart failure, and medications.
Hepatic failure is defined as the occurrence of signs or symptoms of hepatic encephalopathy in a person with severe acute or chronic liver disease. The first signs of hepatic encephalopathy can be subtle and nonspecific—change in sleep patterns, change in personality, irritability, and mental dullness. Thereafter, confusion, disorientation, stupor, and eventually coma supervene. In acute liver failure, excitability and mania may be present. Physical findings include asterixis and flapping tremors of the body and tongue. Fetor hepaticus refers to the slightly sweet, ammoniacal odor that can develop in patients with liver failure, particularly if there is portal-venous shunting of blood around the liver. Other causes of coma and disorientation should be excluded, mainly electrolyte imbalances, sedative use, and renal or respiratory failure. The appearance of hepatic encephalopathy during acute hepatitis is the major criterion for diagnosis of fulminant hepatitis and indicates a poor prognosis. In chronic liver disease, encephalopathy is usually triggered by a medical complication such as gastrointestinal bleeding, over-diuresis, uremia, dehydration, electrolyte imbalance, infection, constipation, or use of narcotic analgesics.
A helpful measure of hepatic encephalopathy is a careful mental-status examination and use of the trail-making test, which consists of a series of 25 numbered circles that the patient is asked to connect as rapidly as possible using a pencil. The normal range for the connect-the-dot test is 15–30 sec; it is considerably longer in patients with early hepatic encephalopathy. Other tests include drawing of abstract objects or comparison of a signature to previous examples. More sophisticated testing—e.g., with electroencephalography and visual evoked potentials—can detect mild forms of encephalopathy but are rarely clinically useful.
Other signs of advanced liver disease include umbilical hernia from ascites, hydrothorax, prominent veins over the abdomen, and caput medusa, a condition that consists of collateral veins radiating from the umbilicus and results from recanulation of the umbilical vein. Widened pulse pressure and signs of a hyperdynamic circulation can occur in patients with cirrhosis as a result of fluid and sodium retention, increased cardiac output, and reduced peripheral resistance. Patients with long-standing cirrhosis and portal hypertension are prone to develop the hepatopulmonary syndrome, which is defined by the triad of liver disease, hypoxemia, and pulmonary arteriovenous shunting. The hepatopulmonary syndrome is characterized by platypnea and orthodeoxia: shortness of breath and oxygen desaturation that occur paradoxically upon the assumption of an upright position. Measurement of oxygen saturation by pulse oximetry is a reliable screening test for hepatopulmonary syndrome.
Several skin disorders and changes are common in liver disease. Hyperpigmentation is typical of advanced chronic cholestatic diseases such as primary biliary cirrhosis and sclerosing cholangitis. In these same conditions, xanthelasma and tendon xanthomata occur as a result of retention and high serum levels of lipids and cholesterol. Slate-gray pigmentation of the skin is also seen with hemochromatosis if iron levels are high for a prolonged period. Mucocutaneous vasculitis with palpable purpura, especially on the lower extremities, is typical of cryoglobulinemia of chronic hepatitis C but can also occur in chronic hepatitis B.
Some physical signs point to specific liver diseases. Kayser-Fleischer rings occur in Wilson’s disease and consist of a golden-brown copper pigment deposited in Descemet’s membrane at the periphery of the cornea; they are best seen by slit-lamp examination. Dupuytren contracture and parotid enlargement are suggestive of chronic alcoholism and alcoholic liver disease. In metastatic liver disease or primary hepatocellular carcinoma, signs of cachexia and wasting as well as firm hepatomegaly and a hepatic bruit may be prominent.
DIAGNOSIS OF LIVER DISEASE
The major causes of liver disease and key diagnostic features are outlined in Table 357-3, and an algorithm for evaluation of the patient with suspected liver disease is shown in Fig. 357-1. Specifics of diagnosis are discussed in later chapters. The most common causes of acute liver disease are viral hepatitis (particularly hepatitis A, B, and C), drug-induced liver injury, cholangitis, and alcoholic liver disease. Liver biopsy usually is not needed in the diagnosis and management of acute liver disease, exceptions being situations where the diagnosis remains unclear despite thorough clinical and laboratory investigation. Liver biopsy can be helpful in diagnosing drug-induced liver disease and acute alcoholic hepatitis.
IMPORTANT DIAGNOSTIC TESTS IN COMMON LIVER DISEASES |
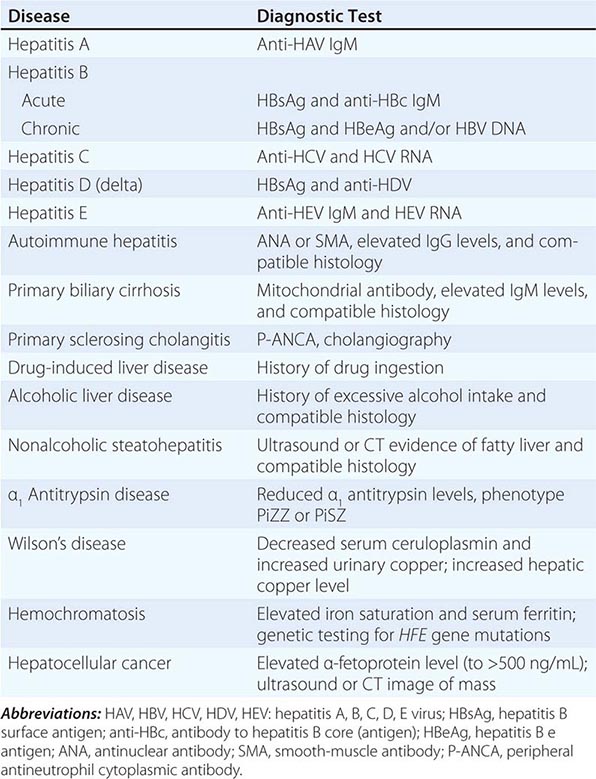
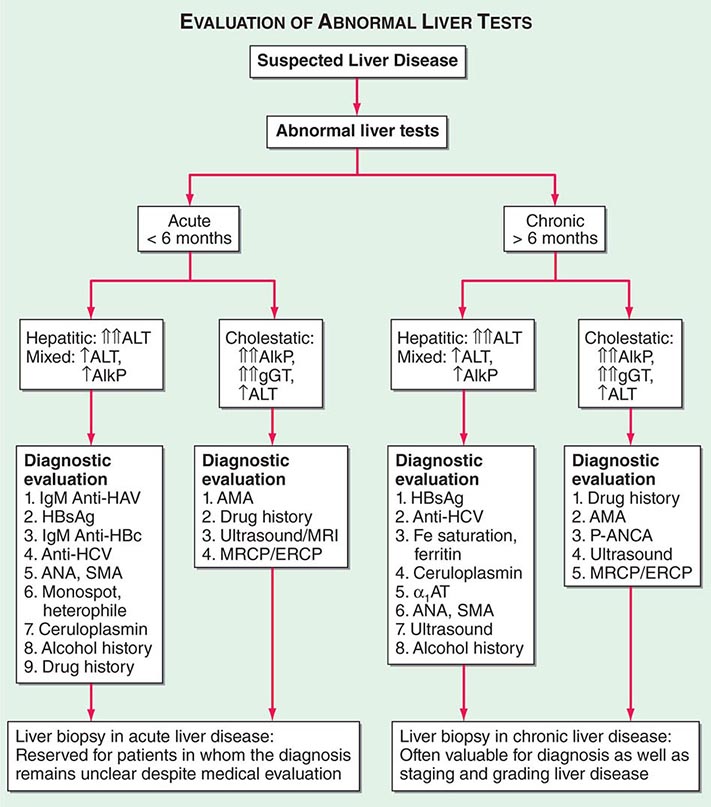
FIGURE 357-1 Algorithm for evaluation of abnormal liver tests. For patients with suspected liver disease, an appropriate approach to evaluation is initial routine liver testing—e.g., measurement of serum bilirubin, albumin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase (AlkP). These results (sometimes complemented by testing of γ-glutamyl transpeptidase; gGT) will establish whether the pattern of abnormalities is hepatic, cholestatic, or mixed. In addition, the duration of symptoms or abnormalities will indicate whether the disease is acute or chronic. If the disease is acute and if history, laboratory tests, and imaging studies do not reveal a diagnosis, liver biopsy is appropriate to help establish the diagnosis. If the disease is chronic, liver biopsy can be helpful not only for diagnosis but also for grading of the activity and staging the progression of disease. This approach is generally applicable to patients without immune deficiency. In patients with HIV infection or recipients of bone marrow or solid organ transplants, the diagnostic evaluation should also include evaluation for opportunistic infections (e.g., with adenovirus, cytomegalovirus, Coccidioides, hepatitis E virus) as well as for vascular and immunologic conditions (veno-occlusive disease, graft-versus-host disease). HAV, hepatitis A virus; HCV, hepatitis C virus; HBsAg, hepatitis B surface antigen; anti-HBc, antibody to hepatitis B core (antigen); ANA, antinuclear antibody; SMA, smooth-muscle antibody; MRCP, magnetic resonance cholangiopancreatography; ERCP, endoscopic retrograde cholangiopancreatography; α1 AT, α1 antitrypsin; AMA; antimitochondrial antibody; P-ANCA, peripheral antineutrophil cytoplasmic antibody.
The most common causes of chronic liver disease, in general order of frequency, are chronic hepatitis C, alcoholic liver disease, nonalcoholic steatohepatitis, chronic hepatitis B, autoimmune hepatitis, sclerosing cholangitis, primary biliary cirrhosis, hemochromatosis, and Wilson’s disease. Hepatitis E virus is a rare cause of chronic hepatitis, with cases occurring mostly in persons who are immunosuppressed or immunodeficient. Strict diagnostic criteria have not been developed for most liver diseases, but liver biopsy plays an important role in the diagnosis of autoimmune hepatitis, primary biliary cirrhosis, nonalcoholic and alcoholic steatohepatitis, and Wilson’s disease (with a quantitative hepatic copper level in the last instance).
Laboratory Testing Diagnosis of liver disease is greatly aided by the availability of reliable and sensitive tests of liver injury and function. A typical battery of blood tests used for initial assessment of liver disease includes measurement of levels of serum alanine and aspartate aminotransferases, alkaline phosphatase, direct and total serum bilirubin and albumin, and prothrombin time. The pattern of abnormalities generally points to hepatocellular versus cholestatic liver disease and helps determine whether the disease is acute or chronic and whether cirrhosis and hepatic failure are present. On the basis of these results, further testing over time may be necessary. Other laboratory tests may be helpful, such as γ-glutamyl transpeptidase to define whether alkaline phosphatase elevations are due to liver disease; hepatitis serology to define the type of viral hepatitis; and autoimmune markers to diagnose primary biliary cirrhosis (antimitochondrial antibody), sclerosing cholangitis (peripheral antineutrophil cytoplasmic antibody), and autoimmune hepatitis (antinuclear, smooth-muscle, and liver-kidney microsomal antibody). A simple delineation of laboratory abnormalities and common liver diseases is given in Table 357-3.
The use and interpretation of liver function tests are summarized in Chap. 358.
Diagnostic Imaging Great advances have been made in hepatobiliary imaging, although no method is adequately accurate in demonstrating underlying cirrhosis. Of the many modalities available for imaging the liver, ultrasound, CT, and MRI are the most commonly employed and are complementary to one another. In general, ultrasound and CT are highly sensitive for detecting biliary duct dilation and are the first-line options for investigating cases of suspected obstructive jaundice. All three modalities can detect a fatty liver, which appears bright on imaging studies. Modifications of CT and MRI can be used to quantify liver fat, and this information may ultimately be valuable in monitoring therapy in patients with fatty liver disease. Magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) are the procedures of choice for visualization of the biliary tree. MRCP offers several advantages over ERCP: there is no need for contrast media or ionizing radiation, images can be acquired faster, the procedure is less operator dependent, and it carries no risk of pancreatitis. MRCP is superior to ultrasound and CT for detecting choledocholithiasis but is less specific. MRCP is useful in the diagnosis of bile duct obstruction and congenital biliary abnormalities, but ERCP is more valuable in evaluating ampullary lesions and primary sclerosing cholangitis. ERCP permits biopsy, direct visualization of the ampulla and common bile duct, and intraductal ultrasonography. It also provides several therapeutic options in patients with obstructive jaundice, such as sphincterotomy, stone extraction, and placement of nasobiliary catheters and biliary stents. Doppler ultrasound and MRI are used to assess hepatic vasculature and hemodynamics and to monitor surgically or radiologically placed vascular shunts, including transjugular intrahepatic portosystemic shunts. Multidetector or spiral CT and MRI with contrast-enhancement are the procedures of choice for the identification and evaluation of hepatic masses, the staging of liver tumors, and preoperative assessment. With regard to mass lesions, the sensitivity of hepatic imaging continues to increase; unfortunately, specificity remains a problem, and often two and sometimes three studies are needed before a diagnosis can be reached. Recently, ultrasound transient elastography has been approved for the measurement of hepatic stiffness—providing an indirect assessment of cirrhosis; this technique can eliminate the need for liver biopsy if the only indication is the assessment of disease stage. Magnetic resonance elastography is now undergoing evaluation for its ability to detect different degrees of hepatic fibrosis. Studies are ongoing to determine whether hepatic elastography is an appropriate means of monitoring fibrosis and disease progression. Finally, interventional radiologic techniques allow the biopsy of solitary lesions, the radiofrequency ablation and chemoembolization of cancerous lesions, the insertion of drains into hepatic abscesses, the measurement of portal pressure, and the creation of vascular shunts in patients with portal hypertension. Which modality to use depends on factors such as availability, cost, and experience of the radiologist with each technique.
Liver Biopsy Liver biopsy remains the criterion standard in the evaluation of patients with liver disease, particularly chronic liver disease. Liver biopsy is necessary for diagnosis in selected instances but is more often useful for assessment of the severity (grade) and stage of liver damage, prediction of prognosis, and monitoring of the response to treatment. The size of the liver biopsy sample is an important determinant of reliability; a length of 1.5–2 cm is necessary for accurate assessment of fibrosis. In the future, noninvasive means of assessing disease activity (batteries of blood tests) and fibrosis (elastography and fibrosis markers) may replace liver biopsy for the staging and grading of disease.
GRADING AND STAGING OF LIVER DISEASE
Grading refers to an assessment of the severity or activity of liver disease, whether acute or chronic; active or inactive; and mild, moderate, or severe. Liver biopsy is the most accurate means of assessing severity, particularly in chronic liver disease. Serum aminotransferase levels serve as convenient and noninvasive markers for disease activity but do not always reliably reflect disease severity. Thus, normal serum aminotransferase levels in patients with hepatitis B surface antigen in serum may indicate the inactive carrier state or may reflect mild chronic hepatitis B or hepatitis B with fluctuating disease activity. Serum testing for hepatitis B e antigen and hepatitis B virus DNA can help sort out these different patterns, but these markers can also fluctuate and change over time. Similarly, in chronic hepatitis C, serum aminotransferase levels can be normal despite moderate disease activity. Finally, in both alcoholic and nonalcoholic steatohepatitis, aminotransferase levels are quite unreliable in reflecting severity. In these conditions, liver biopsy is helpful in guiding management and identifying appropriate therapy, particularly if treatment is difficult, prolonged, and expensive, as is often the case in chronic viral hepatitis. Of the several well-verified numerical scales for grading activity in chronic liver disease, the most commonly used are the histology activity index and the Ishak histology scale.
Liver biopsy is also the most accurate means of assessing stage of disease as early or advanced, precirrhotic, and cirrhotic. Staging of disease pertains largely to chronic liver diseases in which progression to cirrhosis and end-stage disease can occur but may require years or decades. Clinical features, biochemical tests, and hepatic imaging studies are helpful in assessing stage but generally become abnormal only in the middle to late stages of cirrhosis. Noninvasive tests that suggest advanced fibrosis include mild elevations of bilirubin, prolongation of prothrombin time, slight decreases in serum albumin, and mild thrombocytopenia (which is often the first indication of worsening fibrosis). Combinations of blood test results have been used to create models for predicting advanced liver disease, but these models are not reliable enough to use on a regular basis and only separate advanced from early disease. Recently, elastography and noninvasive breath tests using 13C-labeled compounds have been proposed as a means of detecting early stages of fibrosis and liver dysfunction, but their reliability and reproducibility remain to be proven. Thus, at present, mild to moderate stages of hepatic fibrosis are detectable only by liver biopsy. In the assessment of stage, the degree of fibrosis is usually used as the quantitative measure. The amount of fibrosis is generally staged on a scale of 0 to 4+ (Metavir scale) or 0 to 6+ (Ishak scale). The importance of staging relates primarily to prognosis and to optimal management of complications. Patients with cirrhosis are candidates for screening and surveillance for esophageal varices and hepatocellular carcinoma. Patients without advanced fibrosis need not undergo screening.
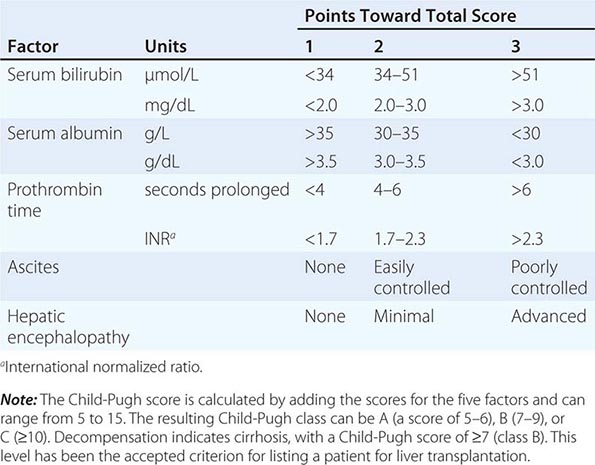
Cirrhosis can also be staged clinically. A reliable staging system is the modified Child-Pugh classification, with a scoring system of 5–15: scores of 5 and 6 represent Child-Pugh class A (consistent with “compensated cirrhosis”), scores of 7–9 represent class B, and scores of 10–15 represent class C (Table 357-4). This scoring system was initially devised to stratify patients into risk groups before portal decompressive surgery. The Child-Pugh score is a reasonably reliable predictor of survival in many liver diseases and predicts the likelihood of major complications of cirrhosis, such as bleeding from varices and spontaneous bacterial peritonitis. This classification scheme was used to assess prognosis in cirrhosis and to provide standard criteria for listing a patient as a candidate for liver transplantation (Child-Pugh class B). Recently, the Child-Pugh system has been replaced by the Model for End-Stage Liver Disease (MELD) system for the latter purpose. The MELD score is a prospectively derived system designed to predict the prognosis of patients with liver disease and portal hypertension. This score is calculated from three noninvasive variables: the prothrombin time expressed as the international normalized ratio (INR), the serum bilirubin level, and the serum creatinine concentration. (http://optn.transplant.hrsa.gov/resources/MeldPeldCalculator.asp?index=98).
CHILD-PUGH CLASSIFICATION OF CIRRHOSIS |
The MELD system provides a more objective means of assessing disease severity and has less center-to-center variation than the Child-Pugh score as well as a wider range of values. MELD is currently used to establish priority listing for liver transplantation in the United States. A similar system, PELD (pediatric end-stage liver disease), is based on bilirubin, INR, serum albumin, age, and nutritional status and is used for children <12 years of age.
Thus, liver biopsy is helpful not only in diagnosis but also in management of chronic liver disease and assessment of prognosis. Because liver biopsy is an invasive procedure and not without complications, it should be used only when it will contribute materially to decisions about management and therapy.
NONSPECIFIC ISSUES IN THE MANAGEMENT OF PATIENTS WITH LIVER DISEASE
Specifics on the management of different forms of acute or chronic liver disease are supplied in subsequent chapters, but certain issues are applicable to any patient with liver disease. These issues include advice regarding alcohol use, medication use, vaccination, and surveillance for complications of liver disease. Alcohol should be used sparingly, if at all, by patients with liver disease. Abstinence from alcohol should be encouraged for all patients with alcohol-related liver disease, patients with cirrhosis, and patients receiving interferon-based therapy for hepatitis B or C. With regard to vaccinations, all patients with liver disease should receive hepatitis A vaccine, and those with risk factors should receive hepatitis B vaccine as well. Influenza and pneumococcal vaccination should also be encouraged, with adherence to the recommendations of the Centers for Disease Control and Prevention. Patients with liver disease should exercise caution in using any medications other than those that are most necessary. Drug-induced hepatotoxicity can mimic many forms of liver disease and can cause exacerbations of chronic hepatitis and cirrhosis; drugs should be suspected in any situation in which the cause of exacerbation is unknown. Finally, consideration should be given to surveillance for complications of chronic liver disease such as variceal hemorrhage and hepatocellular carcinoma. Cirrhosis warrants upper endoscopy to assess the presence of varices, and the patient should receive chronic therapy with beta blockers or should be offered endoscopic obliteration if large varices are found. Moreover, cirrhosis warrants screening and long-term surveillance for development of hepatocellular carcinoma. While the optimal regimen for such surveillance has not been established, an appropriate approach is ultrasound of the liver at 6- to 12-month intervals.
358 | Evaluation of Liver Function |
Several biochemical tests are useful in the evaluation and management of patients with hepatic dysfunction. These tests can be used to (1) detect the presence of liver disease, (2) distinguish among different types of liver disorders, (3) gauge the extent of known liver damage, and (4) follow the response to treatment.
Liver tests have shortcomings. They can be normal in patients with serious liver disease and abnormal in patients with diseases that do not affect the liver. Liver tests rarely suggest a specific diagnosis; rather, they suggest a general category of liver disease, such as hepatocellular or cholestatic, which then further directs the evaluation.
The liver carries out thousands of biochemical functions, most of which cannot be easily measured by blood tests. Laboratory tests measure only a limited number of these functions. In fact, many tests, such as the aminotransferases or alkaline phosphatase, do not measure liver function at all. Rather, they detect liver cell damage or interference with bile flow. Thus, no one test enables the clinician to accurately assess the liver’s total functional capacity.
To increase both the sensitivity and the specificity of laboratory tests in the detection of liver disease, it is best to use them as a battery. Tests usually employed in clinical practice include the bilirubin, aminotransferases, alkaline phosphatase, albumin, and prothrombin time tests. When more than one of these tests provide abnormal findings or the findings are persistently abnormal on serial determinations, the probability of liver disease is high. When all test results are normal, the probability of missing occult liver disease is low.
When evaluating patients with liver disorders, it is helpful to group these tests into general categories as outlined below.
TESTS BASED ON DETOXIFICATION AND EXCRETORY FUNCTIONS
Serum Bilirubin (See also Chap. 58) Bilirubin, a breakdown product of the porphyrin ring of heme-containing proteins, is found in the blood in two fractions—conjugated and unconjugated. The unconjugated fraction, also termed the indirect fraction, is insoluble in water and is bound to albumin in the blood. The conjugated (direct) bilirubin fraction is water soluble and can therefore be excreted by the kidney. When measured by modifications of the original van den Bergh method, normal values of total serum bilirubin are reported between 1 and 1.5 mg/dL with 95% of a normal population falling between 0.2 and 0.9 mg/dL. If the direct-acting fraction is less than 15% of the total, the bilirubin can be considered to all be indirect. The most frequently reported upper limit of normal for conjugated bilirubin is 0.3 mg/dL.
Elevation of the unconjugated fraction of bilirubin is rarely due to liver disease. An isolated elevation of unconjugated bilirubin is seen primarily in hemolytic disorders and in a number of genetic conditions such as Crigler-Najjar and Gilbert’s syndromes (Chap. 58). Isolated unconjugated hyperbilirubinemia (bilirubin elevated but <15% direct) should prompt a workup for hemolysis (Fig. 358-1). In the absence of hemolysis, an isolated, unconjugated hyperbilirubinemia in an otherwise healthy patient can be attributed to Gilbert’s syndrome, and no further evaluation is required.
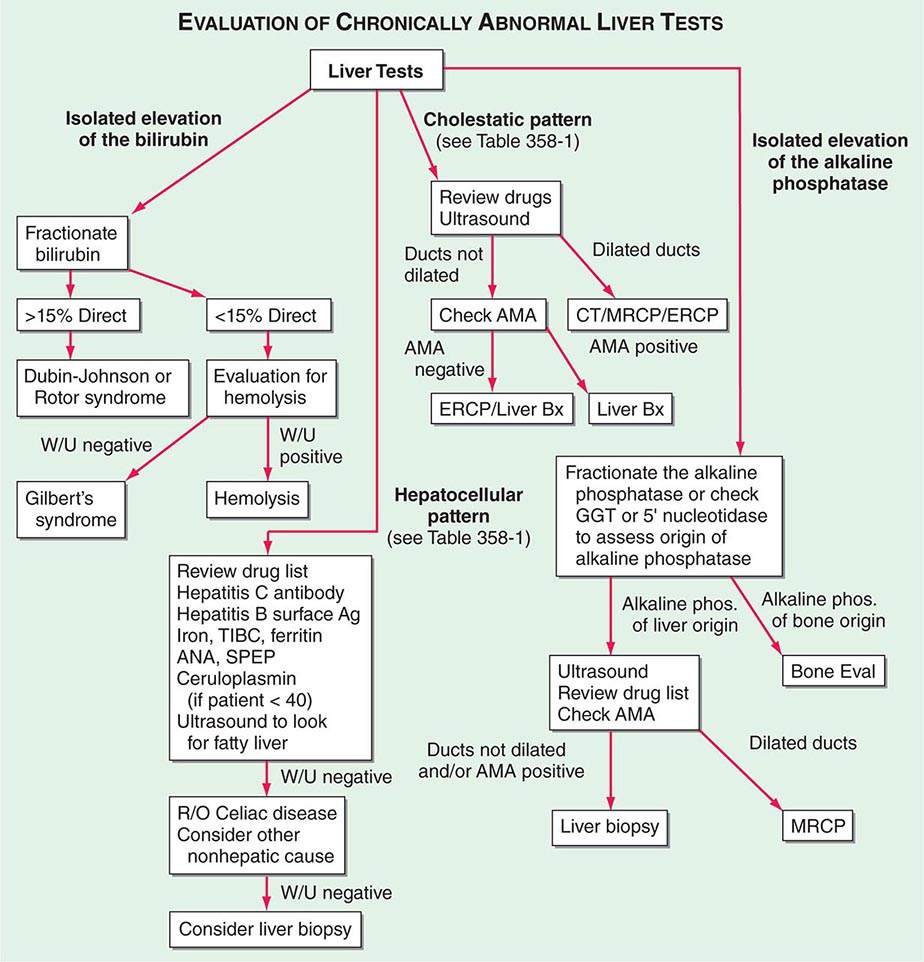
FIGURE 358-1 Algorithm for the evaluation of chronically abnormal liver tests. AMA, antimitochondrial antibody; ANA, antinuclear antibody; Bx, biopsy; CT, computed tomography; ERCP, endoscopic retrograde cholangiopancreatography; GGT, γ glutamyl transpeptidase; MRCP, magnetic resonance cholangiopancreatography; R/O, rule out; SPEP, serum protein electrophoresis; TIBC, total iron-binding capacity; W/U, workup.
In contrast, conjugated hyperbilirubinemia almost always implies liver or biliary tract disease. The rate-limiting step in bilirubin metabolism is not conjugation of bilirubin, but rather the transport of conjugated bilirubin into the bile canaliculi. Thus, elevation of the conjugated fraction may be seen in any type of liver disease. In most liver diseases, both conjugated and unconjugated fractions of the bilirubin tend to be elevated. Except in the presence of a purely unconjugated hyperbilirubinemia, fractionation of the bilirubin is rarely helpful in determining the cause of jaundice.
Although the degree of elevation of the serum bilirubin has not been critically assessed as a prognostic marker, it is important in a number of conditions. In viral hepatitis, the higher the serum bilirubin, the greater is the hepatocellular damage. Total serum bilirubin correlates with poor outcomes in alcoholic hepatitis. It is also a critical component of the Model for End-Stage Liver Disease (MELD) score, a tool used to estimate survival of patients with end-stage liver disease and assess operative risk of patients with cirrhosis. An elevated total serum bilirubin in patients with drug-induced liver disease indicates more severe injury.
Urine Bilirubin Unconjugated bilirubin always binds to albumin in the serum and is not filtered by the kidney. Therefore, any bilirubin found in the urine is conjugated bilirubin; the presence of bilirubinuria implies the presence of liver disease. A urine dipstick test can theoretically give the same information as fractionation of the serum bilirubin. This test is almost 100% accurate. Phenothiazines may give a false-positive reading with the Ictotest tablet. In patients recovering from jaundice, the urine bilirubin clears prior to the serum bilirubin.
Blood Ammonia Ammonia is produced in the body during normal protein metabolism and by intestinal bacteria, primarily those in the colon. The liver plays a role in the detoxification of ammonia by converting it to urea, which is excreted by the kidneys. Striated muscle also plays a role in detoxification of ammonia, where it is combined with glutamic acid to form glutamine. Patients with advanced liver disease typically have significant muscle wasting, which likely contributes to hyperammonemia in these patients. Some physicians use the blood ammonia for detecting encephalopathy or for monitoring hepatic synthetic function, although its use for either of these indications has problems. There is very poor correlation between either the presence or the severity of acute encephalopathy and elevation of blood ammonia; it can be occasionally useful for identifying occult liver disease in patients with mental status changes. There is also a poor correlation of the blood serum ammonia and hepatic function. The ammonia can be elevated in patients with severe portal hypertension and portal blood shunting around the liver even in the presence of normal or near-normal hepatic function. Elevated arterial ammonia levels have been shown to correlate with outcome in fulminant hepatic failure.
Serum Enzymes The liver contains thousands of enzymes, some of which are also present in the serum in very low concentrations. These enzymes have no known function in the serum and behave like other serum proteins. They are distributed in the plasma and in interstitial fluid and have characteristic half-lives, which are usually measured in days. Very little is known about the catabolism of serum enzymes, although they are probably cleared by cells in the reticuloendothelial system. The elevation of a given enzyme activity in the serum is thought to primarily reflect its increased rate of entrance into serum from damaged liver cells.
Serum enzyme tests can be grouped into three categories: (1) enzymes whose elevation in serum reflects damage to hepatocytes, (2) enzymes whose elevation in serum reflects cholestasis, and (3) enzyme tests that do not fit precisely into either pattern.
ENZYMES THAT REFLECT DAMAGE TO HEPATOCYTES The aminotransferases (transaminases) are sensitive indicators of liver cell injury and are most helpful in recognizing acute hepatocellular diseases such as hepatitis. They include aspartate aminotransferase (AST) and alanine aminotransferase (ALT). AST is found in the liver, cardiac muscle, skeletal muscle, kidneys, brain, pancreas, lungs, leukocytes, and erythrocytes in decreasing order of concentration. ALT is found primarily in the liver and is therefore a more specific indicator of liver injury. The aminotransferases are normally present in the serum in low concentrations. These enzymes are released into the blood in greater amounts when there is damage to the liver cell membrane resulting in increased permeability. Liver cell necrosis is not required for the release of the aminotransferases, and there is a poor correlation between the degree of liver cell damage and the level of the aminotransferases. Thus, the absolute elevation of the aminotransferases is of no prognostic significance in acute hepatocellular disorders.
The normal range for aminotransferases varies widely among laboratories, but generally ranges from 10–40 IU/L. The interlaboratory variation in normal range is due to technical reasons; no reference standards exist to establish upper limits of normal for ALT and AST. Some have recommended revisions of normal limits of the aminotransferases to adjust for sex and body mass index, but others have noted the potential costs and unclear benefits of implementing this change.
Any type of liver cell injury can cause modest elevations in the serum aminotransferases. Levels of up to 300 IU/L are nonspecific and may be found in any type of liver disorder. Minimal ALT elevations in asymptomatic blood donors rarely indicate severe liver disease; studies have shown that fatty liver disease is the most likely explanation. Striking elevations—i.e., aminotransferases >1000 IU/L—occur almost exclusively in disorders associated with extensive hepatocellular injury such as (1) viral hepatitis, (2) ischemic liver injury (prolonged hypotension or acute heart failure), or (3) toxin- or drug-induced liver injury.
The pattern of the aminotransferase elevation can be helpful diagnostically. In most acute hepatocellular disorders, the ALT is higher than or equal to the AST. Whereas the AST:ALT ratio is typically <1 in patients with chronic viral hepatitis and nonalcoholic fatty liver disease, a number of groups have noted that as cirrhosis develops, this ratio rises to >1. An AST:ALT ratio >2:1 is suggestive, whereas a ratio >3:1 is highly suggestive, of alcoholic liver disease. The AST in alcoholic liver disease is rarely >300 IU/L, and the ALT is often normal. A low level of ALT in the serum is due to an alcohol-induced deficiency of pyridoxal phosphate.
The aminotransferases are usually not greatly elevated in obstructive jaundice. One notable exception occurs during the acute phase of biliary obstruction caused by the passage of a gallstone into the common bile duct. In this setting, the aminotransferases can briefly be in the 1000–2000 IU/L range. However, aminotransferase levels decrease quickly, and the liver function tests rapidly evolve into those typical of cholestasis.
ENZYMES THAT REFLECT CHOLESTASIS The activities of three enzymes—alkaline phosphatase, 5′-nucleotidase, and γ-glutamyl transpeptidase (GGT)—are usually elevated in cholestasis. Alkaline phosphatase and 5′-nucleotidase are found in or near the bile canalicular membrane of hepatocytes, whereas GGT is located in the endoplasmic reticulum and in bile duct epithelial cells. Reflecting its more diffuse localization in the liver, GGT elevation in serum is less specific for cholestasis than are elevations of alkaline phosphatase or 5′-nucleotidase. Some have advocated the use of GGT to identify patients with occult alcohol use. Its lack of specificity makes its use in this setting questionable.
The normal serum alkaline phosphatase consists of many distinct isoenzymes found in the liver; bone; placenta; and, less commonly, small intestine. Patients over age 60 can have a mildly elevated alkaline phosphatase (1–1.5 times normal), whereas individuals with blood types O and B can have an elevation of the serum alkaline phosphatase after eating a fatty meal due to the influx of intestinal alkaline phosphatase into the blood. It is also nonpathologically elevated in children and adolescents undergoing rapid bone growth because of bone alkaline phosphatase, and late in normal pregnancies due to the influx of placental alkaline phosphatase.
Elevation of liver-derived alkaline phosphatase is not totally specific for cholestasis, and a less than threefold elevation can be seen in almost any type of liver disease. Alkaline phosphatase elevations greater than four times normal occur primarily in patients with cholestatic liver disorders, infiltrative liver diseases such as cancer and amyloidosis, and bone conditions characterized by rapid bone turnover (e.g., Paget’s disease). In bone diseases, the elevation is due to increased amounts of the bone isoenzymes. In liver diseases, the elevation is almost always due to increased amounts of the liver isoenzyme.
If an elevated serum alkaline phosphatase is the only abnormal finding in an apparently healthy person, or if the degree of elevation is higher than expected in the clinical setting, identification of the source of elevated isoenzymes is helpful (Fig. 358-1). This problem can be approached in two ways. First, and most precise, is the fractionation of the alkaline phosphatase by electrophoresis. The second, best substantiated, and most available approach involves the measurement of serum 5′-nucleotidase or GGT. These enzymes are rarely elevated in conditions other than liver disease.
In the absence of jaundice or elevated aminotransferases, an elevated alkaline phosphatase of liver origin often, but not always, suggests early cholestasis and, less often, hepatic infiltration by tumor or granulomata. Other conditions that cause isolated elevations of the alkaline phosphatase include Hodgkin’s disease, diabetes, hyperthyroidism, congestive heart failure, amyloidosis, and inflammatory bowel disease.
The level of serum alkaline phosphatase elevation is not helpful in distinguishing between intrahepatic and extrahepatic cholestasis. There is essentially no difference among the values found in obstructive jaundice due to cancer, common duct stone, sclerosing cholangitis, or bile duct stricture. Values are similarly increased in patients with intrahepatic cholestasis due to drug-induced hepatitis; primary biliary cirrhosis; rejection of transplanted livers; and, rarely, alcohol-induced steatohepatitis. Values are also greatly elevated in hepatobiliary disorders seen in patients with AIDS (e.g., AIDS cholangiopathy due to cytomegalovirus or cryptosporidial infection and tuberculosis with hepatic involvement).
TESTS THAT MEASURE BIOSYNTHETIC FUNCTION OF THE LIVER
Serum Albumin Serum albumin is synthesized exclusively by hepatocytes. Serum albumin has a long half-life: 18–20 days, with ~4% degraded per day. Because of this slow turnover, the serum albumin is not a good indicator of acute or mild hepatic dysfunction; only minimal changes in the serum albumin are seen in acute liver conditions such as viral hepatitis, drug-related hepatotoxicity, and obstructive jaundice. In hepatitis, albumin levels <3 g/dL should raise the possibility of chronic liver disease. Hypoalbuminemia is more common in chronic liver disorders such as cirrhosis and usually reflects severe liver damage and decreased albumin synthesis. One exception is the patient with ascites in whom synthesis may be normal or even increased, but levels are low because of the increased volume of distribution. However, hypoalbuminemia is not specific for liver disease and may occur in protein malnutrition of any cause, as well as protein-losing enteropathies, nephrotic syndrome, and chronic infections that are associated with prolonged increases in levels of serum interleukin 1 and/or tumor necrosis factor, cytokines that inhibit albumin synthesis. Serum albumin should not be measured for screening in patients in whom there is no suspicion of liver disease. A general medical clinic study of consecutive patients in whom no indications were present for albumin measurement showed that although 12% of patients had abnormal test results, the finding was of clinical importance in only 0.4%.
Serum Globulins Serum globulins are a group of proteins made up of γ globulins (immunoglobulins) produced by B lymphocytes and α and β globulins produced primarily in hepatocytes. γ globulins are increased in chronic liver disease, such as chronic hepatitis and cirrhosis. In cirrhosis, the increased serum γ globulin concentration is due to the increased synthesis of antibodies, some of which are directed against intestinal bacteria. This occurs because the cirrhotic liver fails to clear bacterial antigens that normally reach the liver through the hepatic circulation.
Increases in the concentration of specific isotypes of γ globulins are often helpful in the recognition of certain chronic liver diseases. Diffuse polyclonal increases in IgG levels are common in autoimmune hepatitis; increases >100% should alert the clinician to this possibility. Increases in the IgM levels are common in primary biliary cirrhosis, whereas increases in the IgA levels occur in alcoholic liver disease.
COAGULATION FACTORS
With the exception of factor VIII, which is produced by vascular endothelial cells, the blood clotting factors are made exclusively in hepatocytes. Their serum half-lives are much shorter than albumin, ranging from 6 h for factor VII to 5 days for fibrinogen. Because of their rapid turnover, measurement of the clotting factors is the single best acute measure of hepatic synthetic function and helpful in both diagnosis and assessing the prognosis of acute parenchymal liver disease. Useful for this purpose is the serum prothrombin time, which collectively measures factors II, V, VII, and X. Biosynthesis of factors II, VII, IX, and × depends on vitamin K. The international normalized ratio (INR) is used to express the degree of anticoagulation on warfarin therapy. The INR standardizes prothrombin time measurement according to the characteristics of the thromboplastin reagent used in a particular lab, which is expressed as an International Sensitivity Index (ISI); the ISI is then used in calculating the INR.
The prothrombin time may be elevated in hepatitis and cirrhosis as well as in disorders that lead to vitamin K deficiency such as obstructive jaundice or fat malabsorption of any kind. Marked prolongation of the prothrombin time, >5 s above control and not corrected by parenteral vitamin K administration, is a poor prognostic sign in acute viral hepatitis and other acute and chronic liver diseases. The INR, along with the total serum bilirubin and creatinine, are components of the MELD score, which is used as a measure of hepatic decompensation and to allocate organs for liver transplantation.
OTHER DIAGNOSTIC TESTS
Although tests may direct the physician to a category of liver disease, additional radiologic testing and procedures are often necessary to make the proper diagnosis, as shown in Fig. 358-1. The most commonly used ancillary tests are reviewed here, as are the noninvasive tests available for assessing hepatic fibrosis.
Percutaneous Liver Biopsy Percutaneous biopsy of the liver is a safe procedure that can be easily performed at the bedside with local anesthesia and ultrasound guidance. Liver biopsy is of proven value in the following situations: (1) hepatocellular disease of uncertain cause, (2) prolonged hepatitis with the possibility of autoimmune hepatitis, (3) unexplained hepatomegaly, (4) unexplained splenomegaly, (5) hepatic filling defects by radiologic imaging, (6) fever of unknown origin, (7) and staging of malignant lymphoma. Liver biopsy is most accurate in disorders causing diffuse changes throughout the liver and is subject to sampling error in focal infiltrative disorders such as hepatic metastases. Liver biopsy should not be the initial procedure in the diagnosis of cholestasis. The biliary tree should first be assessed for signs of obstruction. Contraindications to performing a percutaneous liver biopsy include significant ascites and prolonged INR. Under these circumstances, the biopsy can be performed via the transjugular approach.
Noninvasive Tests to Detect Hepatic Fibrosis Although liver biopsy is the standard for the assessment of hepatic fibrosis, noninvasive measures of hepatic fibrosis have been developed and show promise. These measures include multiparameter tests aimed at detecting and staging the degree of hepatic fibrosis and imaging techniques. FibroTest (marketed as FibroSure in the United States) is the best evaluated of the multiparameter blood tests. The test incorporates haptoglobin, bilirubin, GGT, apolipoprotein A-I, and α2-macroglobulin and has been found to have high positive and negative predictive values for diagnosing advanced fibrosis in patients with chronic hepatitis C, chronic hepatitis B, and alcoholic liver disease and patients taking methotrexate for psoriasis. Transient elastography (TE), marketed as FibroScan, and magnetic resonance elastography (MRE) both have gained U.S. Food and Drug Administration approval for use in the management of patients with liver disease. TE uses ultrasound waves to measure hepatic stiffness noninvasively. TE has been shown to be accurate for identifying advanced fibrosis in patients with chronic hepatitis C, primary biliary cirrhosis, hemochromatosis, nonalcoholic fatty liver disease, and recurrent chronic hepatitis after liver transplantation. MRE has been found to be superior to TE for staging liver fibrosis in patients with a variety of chronic liver diseases, but requires access to a magnetic resonance imaging scanner.
Ultrasonography Ultrasonography is the first diagnostic test to use in patients whose liver tests suggest cholestasis, to look for the presence of a dilated intrahepatic or extrahepatic biliary tree or to identify gallstones. In addition, it shows space-occupying lesions within the liver, enables the clinician to distinguish between cystic and solid masses, and helps direct percutaneous biopsies. Ultrasound with Doppler imaging can detect the patency of the portal vein, hepatic artery, and hepatic veins and determine the direction of blood flow. This is the first test ordered in patients suspected of having Budd-Chiari syndrome.
USE OF LIVER TESTS
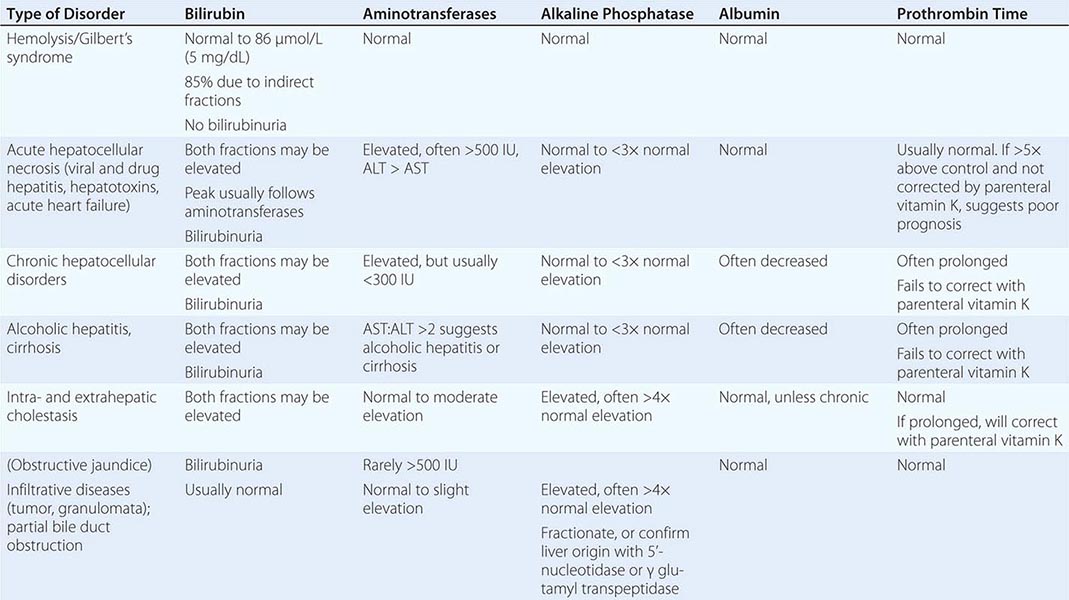
As previously noted, the best way to increase the sensitivity and specificity of laboratory tests in the detection of liver disease is to employ a battery of tests that includes the aminotransferases, alkaline phosphatase, bilirubin, albumin, and prothrombin time along with the judicious use of the other tests described in this chapter. Table 358-1 shows how patterns of liver tests can lead the clinician to a category of disease that will direct further evaluation. However, it is important to remember that no single set of liver tests will necessarily provide a diagnosis. It is often necessary to repeat these tests on several occasions over days to weeks for a diagnostic pattern to emerge. Figure 358-1 is an algorithm for the evaluation of chronically abnormal liver tests.
LIVER TEST PATTERNS IN HEPATOBILIARY DISORDERS |
GLOBAL CONSIDERATIONS
![]() The tests and principles presented in this chapter are applicable worldwide. The causes of liver test abnormalities vary according to region. In developing nations, infectious diseases are more commonly the etiology of abnormal serum liver tests than in developed nations.
The tests and principles presented in this chapter are applicable worldwide. The causes of liver test abnormalities vary according to region. In developing nations, infectious diseases are more commonly the etiology of abnormal serum liver tests than in developed nations.
ACKNOWLEDGMENT
This chapter represents a revised version of a chapter in previous editions of Harrison’s in which Marshall M. Kaplan was a co-author.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


