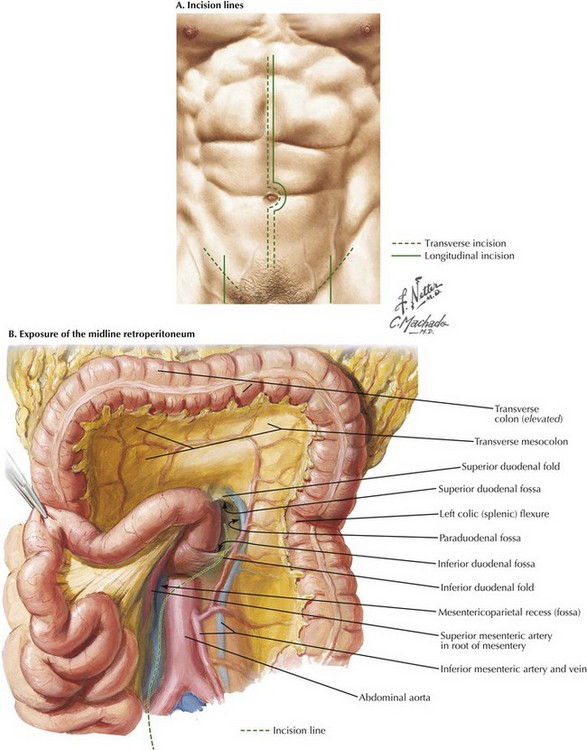
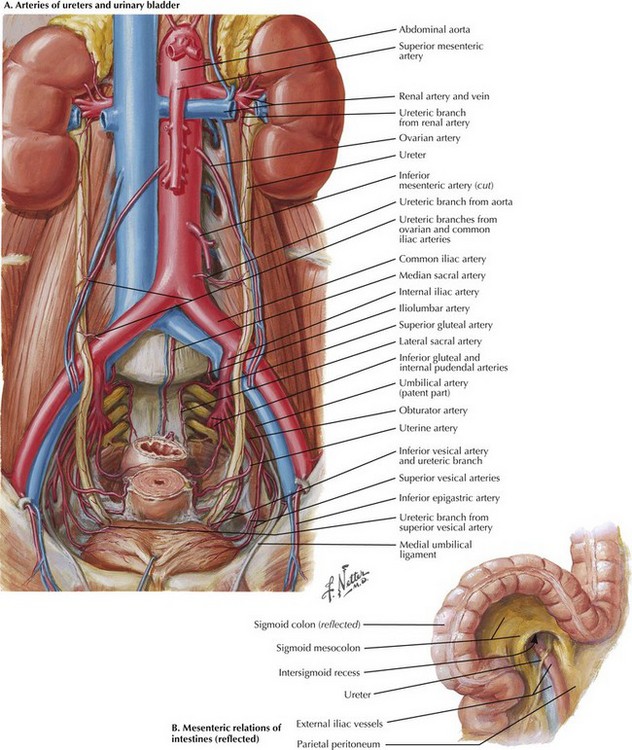
Chapter 33 To begin the operation, the patient is placed on the operating room table in a supine position. A midline abdominal incision is made from the xiphoid process to below the umbilicus for an appropriate distance (Fig. 33-1, A). An AF2 or AAA not involving the common iliac arteries, and for which a predetermined tube graft will be performed, is sufficiently exposed with a shorter abdominal incision. If groin incisions will be used, the groin is opened first in the patient with no previous abdominal incision, with minimal difficulty predicted in exposing the abdominal aorta. A midline incision is made as illustrated in Figure 33-1. The small bowel is moved to the right and superiorly in the abdomen, and the sigmoid colon is gently retracted to the left. These maneuvers expose the midline retroperitoneum, and depending on the patient’s body mass index (BMI), retroperitoneal structures can be easily identified or obscured by retroperitoneal fat (Fig. 33-1, B). Palpation of the aortic bifurcation identifies the midline, and the author incises the pelvic retroperitoneum either in the midline or slightly to the right. This approach allows the surgeon to dissect the right common iliac bifurcation, retracting the peritoneum and its attached fat to the right. Remember that the ureter crosses the iliac vessels anteriorly and at the level of the common iliac bifurcation bilaterally (Fig. 33-2, A). Depending on the level of bypass, vessel loops can be placed around the right external and internal iliac arteries or around the distal common iliac artery, respecting the intimate relationship between the iliac arteries and veins. The most common atherosclerotic pattern demonstrates disease at the distal common iliac artery, so vessel loops around the external and internal iliac arteries are preferred. The vessels are usually soft at this location and will provide the most flexibility in constructing the anastomosis.
Aortic Exposure from the Midline Abdomen

Incisional Anatomy
Iliac Exposure
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine