http://evolve.elsevier.com/McCuistion/pharmacology
Central nervous system (CNS) depressants used to manage symptoms of psychosis and anxiety disorders include antipsychotics and anxiolytics, which may cause psychosis. Antipsychotics are also known as neuroleptics or psychotropics, but the preferred name for this group is either antipsychotics or neuroleptics. The term neuroleptic refers to any drug that modifies psychotic behavior and exerts an antipsychotic effect. Anxiolytics are also called antianxiety drugs or sedative-hypnotics. Certain anxiolytics are used to treat sleep disorders, seizures, and withdrawal symptoms from alcohol or other abuse substances. Some of these drugs are also used for conscious sedation and anesthesia supplementation. However, the anxiolytics described in this chapter are used specifically to treat anxiety and psychotic behaviors.
Psychosis
Psychosis, or loss of contact with reality, is manifested in a variety of mental or psychiatric disorders. Psychosis is usually characterized by more than one symptom, such as difficulty in processing information, disorganized thoughts, distortion of reality, delusions, hallucinations, incoherence, catatonia, and aggressive or violent behavior. Schizophrenia, a chronic psychotic disorder, is the major category of psychosis in which many of these symptoms are manifested.
The symptoms of schizophrenia usually develop in adolescence or early adulthood and are divided into three groups: (1) cognitive symptoms, (2) positive symptoms, and (3) negative symptoms. Cognitive symptoms are characterized by disorganized thinking, memory difficulty, and decreased ability to focus attention. Positive symptoms may be characterized by exaggeration of normal function (e.g., agitation), incoherent speech, hallucinations, delusions, and paranoia. Negative symptoms are characterized by a decrease or loss in function and motivation. A poverty or simplicity of speech, blunted affect, inertia, poor self-care, and social withdrawal are apparent. Negative symptoms tend to be more chronic and persistent. The typical, conventional, or traditional group of antipsychotics (first-generation antipsychotics) is more helpful for managing positive symptoms. A group of antipsychotics called atypical (second-generation antipsychotics) has been found to be the newest treatment for both positive and negative symptoms of schizophrenia.
Antipsychotics compose the largest group of drugs used to treat mental illness. Specifically, these drugs improve the thought processes and behavior of patients with psychotic symptoms, especially those with schizophrenia and other psychotic disorders. They are not used as a primary treatment for anxiety or depression. The theory is that psychotic symptoms result from an imbalance in the neurotransmitter dopamine in the brain. Sometimes these antipsychotics are called dopamine antagonists. Antipsychotics block D2 dopamine receptors in the brain and thus reduce psychotic symptoms. Many antipsychotics block the chemoreceptor trigger zone (CTZ) and vomiting (emetic) center in the brain, producing an antiemetic (prevents or relieves nausea and vomiting) effect. However, when dopamine is blocked, symptoms of extrapyramidal syndrome (EPS) or parkinsonism (a chronic neurologic disorder that affects the extrapyramidal motor tract) such as tremors, masklike facies, rigidity, and shuffling gait may develop. Many patients who take high-potency antipsychotic drugs may require long-term medication for symptoms of parkinsonism.
Antipsychotic Agents
Antipsychotics are divided into two major categories: typical and atypical. The typical antipsychotics, introduced in 1952, are subdivided into phenothiazines and nonphenothiazines. Nonphenothiazines include butyrophenones, dibenzoxazepines, dihydroindolones, and thioxanthenes. The butyrophenones block only the neurotransmitter dopamine. The phenothiazines and the thioxanthenes block norepinephrine, causing sedative and hypotensive effects early in treatment.
Atypical antipsychotics make up the second category of antipsychotics. Clozapine, discovered in the 1960s and made available in Europe in 1971, was the first atypical antipsychotic agent. It was not marketed in the United States until 1990 because of adverse hematologic reactions. Atypical antipsychotics are effective for treating schizophrenia and other psychotic disorders in patients who do not respond to or are intolerant of typical antipsychotics. Because of their decreased side effects, atypical antipsychotics are often used instead of traditional typical antipsychotics as first-line therapy.
Pharmacophysiologic Mechanisms of Action
Antipsychotics block the actions of dopamine and thus may be classified as dopaminergic antagonists. There are five subtypes of dopamine receptors numbered D1 through D5. All antipsychotics block the D2 (dopaminergic) receptor, which in turn promotes the presence of EPS, resulting in drug-induced pseudoparkinsonism in varying degrees. Atypical antipsychotics have a weak affinity to D2 receptors and a stronger affinity to D4 receptors, and they block the serotonin receptor. These agents cause fewer EPS than the typical (phenothiazine) antipsychotic agents, which have a strong affinity to D2 receptors.
Adverse Reactions
Extrapyramidal Syndrome
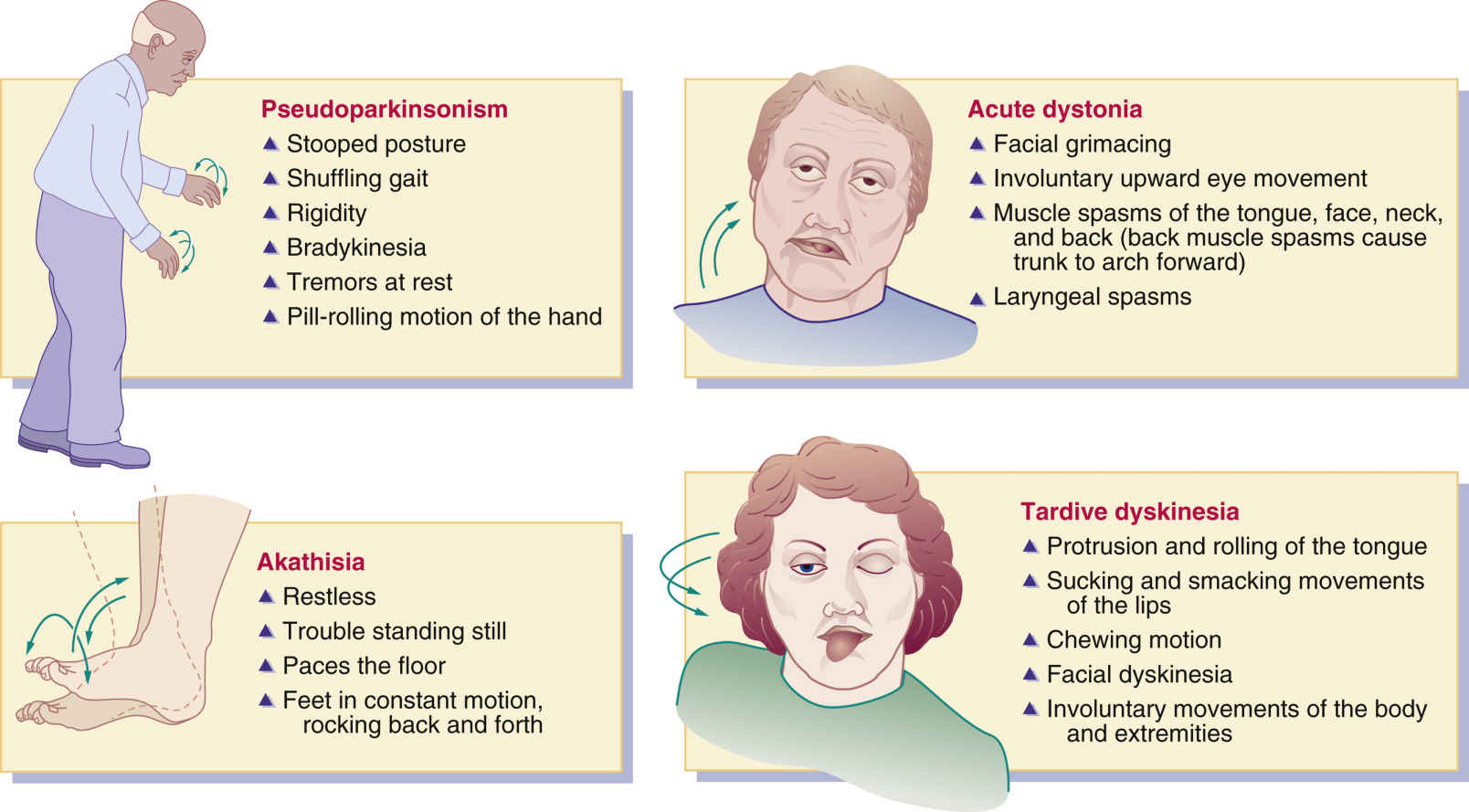
Pseudoparkinsonism, which resembles symptoms of parkinsonism, is a major side effect of typical antipsychotic drugs. Symptoms of pseudoparkinsonism or EPS include stooped posture, masklike facies, rigidity, tremors at rest, shuffling gait, pill-rolling motions of the hands, and bradykinesia. When patients take high-potency typical antipsychotic drugs for extended periods, EPS is more pronounced. Patients who take low-strength antipsychotics such as chlorpromazine are not as likely to have symptoms of pseudoparkinsonism as those who take fluphenazine.
During early treatment with typical antipsychotic agents for schizophrenia and other psychotic disorders, two adverse extrapyramidal reactions that may occur are acute dystonia and akathisia. Tardive dyskinesia is a later phase of extrapyramidal reaction to antipsychotics. Use of anticholinergic drugs helps decrease pseudoparkinsonism symptoms, acute dystonia, and akathisia but has little effect on alleviating tardive dyskinesia. Complementary and Alternative Therapies 22.1 details interactions with antipsychotic agents.

The symptoms of acute dystonia usually occur in 5% of patients within days of taking typical antipsychotics. Characteristics of the reaction include muscle spasms of the face, tongue, neck, and back; facial grimacing; abnormal or involuntary upward eye movement; and laryngeal spasms that can impair respiration. This condition is treated with an anticholinergic antiparkinson drug such as benztropine. The benzodiazepine lorazepam may also be prescribed.
Akathisia occurs in approximately 20% of patients who take a typical antipsychotic drug. With this reaction, the patient has trouble standing still, is restless, paces the floor, and is in constant motion (e.g., rocks back and forth). Akathisia is best treated with a benzodiazepine such as lorazepam or a beta blocker such as propranolol.
Tardive dyskinesia is a serious adverse reaction that occurs in approximately 20% to 30% of patients who have taken a typical antipsychotic drug for more than 1 year. The prevalence is higher in cigarette smokers. The likelihood of developing tardive dyskinesia depends on the dose and duration of the antipsychotic factor. Characteristics of tardive dyskinesia include protrusion and rolling of the tongue, sucking and smacking movements of the lips, chewing motion, and involuntary movement of the body and extremities. In older adults, these reactions are more frequent and severe. The antipsychotic drug should be stopped in all who experience tardive dyskinesia, and another antipsychotic agent should be substituted. Benzodiazepines, calcium channel blockers, and beta blockers are sometimes helpful in decreasing tardive dyskinesia, although no one agent is effective for all patients. High doses of vitamin E may be helpful, and its use to treat tardive dyskinesia is currently under investigation. Clozapine has also been effective for treating tardive dyskinesia. Tetrabenazine, used to improve symptoms of Huntington disease, seems to be effective in treating tardive dyskinesia. Tetrabenazine reduces dopamine, norepinephrine, and serotonin levels. Amantadine has also been helpful in reducing drug-induced involuntary movements. Fig. 22.1 shows the characteristics of pseudoparkinsonism, acute dystonia, akathisia, and tardive dyskinesia.
Neuroleptic Malignant Syndrome
Neuroleptic malignant syndrome (NMS) is a rare but potentially fatal condition associated with antipsychotic drugs. Predisposing factors include excess agitation, exhaustion, and dehydration. NMS symptoms involve muscle rigidity, hyperthermia, altered mental status, profuse diaphoresis, blood pressure fluctuations, tachycardia, dysrhythmias, seizures, rhabdomyolysis, acute renal failure, respiratory failure, and coma. Treatment of NMS involves immediate withdrawal of antipsychotics, adequate hydration, hypothermic blankets, and administration of antipyretics, benzodiazepines, and muscle relaxants such as dantrolene.
Phenothiazines
Chlorpromazine hydrochloride was the first phenothiazine introduced for treating psychotic behavior in patients in psychiatric hospitals. The phenothiazines are subdivided into three groups: aliphatic, piperazine, and piperidine, which differ mostly in their side effects.
The aliphatic phenothiazines produce a strong sedative effect, decreased blood pressure, and may cause moderate EPS (pseudoparkinsonism). Chlorpromazine hydrochloride is in the aliphatic group and may produce pronounced orthostatic hypotension, low blood pressure that occurs when an individual assumes an upright position from a supine position.
The piperazine phenothiazines produce more EPS than other phenothiazines. They also cause dry mouth, urinary retention, and agranulocytosis. Examples of piperazine phenothiazines are fluphenazine and perphenazine.
The piperidine phenothiazines have a strong sedative effect, cause few EPS, have a low to moderate effect on blood pressure, and have no antiemetic effect. Thioridazine is an example of piperidine phenothiazines. Table 22.1 summarizes the effects of the phenothiazines.
Most antipsychotics can be given orally (tablet or liquid), intramuscularly (IM), or intravenously (IV). For oral use, the liquid form might be preferred because some patients may hide tablets in their cheek or under their tongue to avoid taking them. Mouth checks are necessary for noncompliant patients. In addition, the absorption rate is faster with the liquid form, and a peak serum drug level occurs in 2 to 3 hours. The antipsychotics are highly protein bound (>90%), and excretion of the drugs and their metabolites is slow. Phenothiazines are metabolized by liver enzymes into phenothiazine metabolites. Metabolites can be detected in the urine several months after the medication has been discontinued. Phenothiazine metabolites may cause a harmless pinkish to red-brown urine color. The full therapeutic effects of oral antipsychotics may not be evident for 3 to 6 weeks following initiation of therapy, but an observable therapeutic response may be apparent after 7 to 10 days.
Noncompliance with antipsychotics is common. Medication teaching in the following areas is of utmost importance: (1) encourage the patient to take the medication as prescribed, (2) explain and emphasize essential information to compensate for the patient’s knowledge deficit, and (3) provide an interpreter for patients whose first language is not English.
Prototype Drug Chart 22.1 shows the drug characteristics of fluphenazine, a phenothiazine antipsychotic used to manage psychosis. Box 22.1 shows the symptoms and suggested treatment for overdose of phenothiazines.
Pharmacokinetics
Oral absorption of fluphenazine is rapid and unaffected by food. This drug is strongly protein bound and has a long half-life, therefore the drug may accumulate in the body. Fluphenazine is metabolized by the liver, crosses the blood-brain barrier and placenta, and is excreted as metabolites primarily in the urine. With hepatic dysfunction, the phenothiazine dose may need to be decreased. Lack of drug metabolism in the liver will cause an elevation in serum drug level.
Pharmacodynamics
Fluphenazine is prescribed primarily for psychotic disorders. This drug has anticholinergic properties and should be cautiously administered to patients with glaucoma, especially narrow-angle glaucoma. Because hypotension is a side effect of these phenothiazines, any antihypertensives simultaneously administered can cause an additive hypotensive effect. Narcotics and sedative-hypnotics administered simultaneously with these phenothiazines can cause an additive CNS depression. Antacids decrease the absorption rate of both drugs and all phenothiazines, so they should be given 1 hour before or 2 hours after an oral phenothiazine.

The onset of action for fluphenazine hydrochloride is 1 hour, with a duration rate of 6 to 8 hours. Fluphenazine decanoate has delayed absorption, with an onset of action of 24 hours and a duration of 4 weeks.
Nonphenothiazines
The many groups of nonphenothiazine antipsychotics include butyrophenones, dibenzoxazepines, dihydroindolones, and thioxanthenes.
In the butyrophenone group, a frequently prescribed nonphenothiazine is haloperidol. Haloperidol’s pharmacologic behavior is similar to that of the phenothiazines. It is a potent antipsychotic drug in which the equivalent prescribed dose is smaller than that of drugs of lower potency, such as chlorpromazine. The drug dose for haloperidol is 0.5 to 5 mg, whereas the drug dose for chlorpromazine is 10 to 25 mg. Long-acting preparations of haloperidol decanoate and fluphenazine decanoate are given for slow release via injection every 2 to 4 weeks. Administration precautions should be taken to prevent soreness and inflammation at the injection site. Because the medication is a viscous liquid, a large-gauge needle (e.g., 21 gauge) should be used with the Z-track method for administration in a deep muscle; Chapter 10 provides further explanation of the Z-track method of injection. The injection site should not be massaged, and sites should be rotated. These medications should not remain in a plastic syringe longer than 15 minutes. Prototype Drug Chart 22.2 provides the drug data related to haloperidol.
Pharmacokinetics
Haloperidol is absorbed well through the gastrointestinal (GI) mucosa. It has a long half-life and is highly protein bound, so the drug may accumulate. Haloperidol is metabolized in the liver and is excreted in urine and feces.
Pharmacodynamics
Haloperidol alters the effects of dopamine by blocking dopamine receptors, thus sedation and EPS may occur. The drug is used to control psychosis and to decrease agitation in adults and children. Dosages need to be decreased in older adults because of decreased liver function and potential side effects. Haloperidol may be prescribed for children with hyperactive behavior. Because it has anticholinergic activity, care should be taken when administering it to patients with a history of glaucoma.
Haloperidol has a similar onset of action, peak time of concentration, and duration of action as the phenothiazines. It has strong EPS effects. Skin and sun protection is necessary for prolonged use because of the possible side effect of photosensitivity.

From the dibenzoxazepine group, loxapine is a moderately potent agent. It has moderate sedative and orthostatic hypotensive effects and strong EPS effects.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


