Chapter 49 It is important to understand that psychosis is not a disease. Psychosis is the term that is used to describe a general symptom complex in which gross impairment of reality is demonstrated. It has many causes—both organic and psychiatric. Box 49-1 lists symptoms that are commonly associated with the presentation of a clinical psychosis. Table 49-1 shows the most common medical disorders that may present with psychiatric symptoms, but not all of these represent psychotic symptoms. A large number of diverse and even common medications can cause psychotic symptoms (Table 49-2). Table 49-3 lists different psychiatric disorders that may present with psychosis. Therefore, it is difficult to talk about treating the general symptoms of psychosis; it is more productive to talk about specific psychotic disorders such as schizophrenia. TABLE 49-1 Medical Conditions Associated with Psychiatric Symptoms Modified from Gabbard GO: Gabbard’s treatment of psychiatric disorders,ed 4, New York, 2007, American Psychiatric Publishing. TABLE 49-2 Medications That Can Cause Psychotic Symptoms Acyclovir Amantadine Amphetamine-like drugs Anabolic steroids Anticholinergics and atropine Anticonvulsants Antidepressants, all Baclofen Barbiturates Benzodiazepines α-Adrenergic blockers Calcium channel blockers Cephalosporins Corticosteroids Dopamine receptor agonists fluoroquinolone antibiotics Histamine H1-receptor blockers Histamine H2-receptor blockers HMG-CoA reductase inhibitors (statins) NSAIDs Opioids Procaine derivatives Salicylates Sulfonamides Data from The Medical Letter: Some drugs that cause psychiatric symptoms, Med Lett 44:1134, 2002, and Gabbard GO: Gabbard’s treatment of psychiatric disorders, ed 4, New York, 2007, American Psychiatric Publishing. TABLE 49-3 Psychiatric Disorders That May Present with Psychosis Modified from Stern TA et al: Massachusetts General Hospital handbook of general hospital psychiatry,ed 5, St Louis, 2004, Mosby. Schizophrenia is diagnosed by history after the patient is assessed in three areas: 1. Characteristic symptoms: Two of more of the following: 2. Social or occupational dysfunction, notably problems with work, school, interpersonal relations, or self-care 1. Has a reversible organic or substance-induced cause of psychosis been ruled out? 2. Are cognitive deficits prominent? (i.e., delirium or dementia) 3. Is the psychotic illness continuous or episodic? Have psychotic symptoms (active phase) been present for at least 4 weeks? Has evidence of the illness been present for at least 6 months? Is a decline in level of functioning evident? Are negative symptoms present? 4. Are mood episodes prominent? Have episodes of major depression or mania occurred? Do psychotic features occur only during affective episodes? The exact mechanism of antipsychotic drug action is unknown. These drugs are thought to work by blocking postsynaptic dopamine receptors in the hypothalamus, basal ganglia, limbic system, brainstem, and medulla, and to some extent serotonin receptors. Much work has been done to elucidate which receptors each drug affects. How this receptor blocking causes specific changes in behavior and cognition is not known. See Table 49-4 for specific neurotransmitter-receptor blocking actions of individual medications. Each neurotransmitter is associated with specific side effects. However, the correlation between the two is not completely understood. A very complicated and overlapping set of mechanisms interact to produce a wide variety of effects. Another complication is that these drugs produce different effects from patient to patient. Most cause sedation in some people and agitation in others (Box 49-2). Some antipsychotic drugs cause metabolic side effects such as obesity and diabetes by activating the SMAD3 protein, which plays a role in the transforming growth factor beta pathway—a cellular mechanism responsible for inflammation and insulin signaling, among other processes. TABLE 49-4 Comparison of Mechanism of Action and Associated Adverse Reactions
Antipsychotics
Class
Subclass
Generic Name
Trade Name
FIRST GENERATION
Phenothiazines
Aliphatics
chlorpromazine 
Thorazine
Piperazines
fluphenazine
Prolixin
perphenazine
Trilafon
prochlorperazine
Compazine
trifluoperazine
Stelazine
Piperidines
mesoridazine
Serentil
thioridazine
Mellaril
Thioxanthenes
thiothixene
Navane
Phenylbutylpiperadines
Butyrophenones
haloperidol
Haldol
SECOND GENERATION
Dibenzepins
Dibenzodiazepines
clozapine
Clozaril
Benzisoxazoles
Benzisoxazoles
risperidone 
Risperdal, Consta
iloperidone
Fanapt
paliperidone
Invega
Sustena
Thienobenzodiazepines
olanzapine
Zyprexa
Relprevv
Zydis
Dibenzothiazepines
quetiapine
Seroquel 
Seroquel XR 
Benzylisothiazols/piperazines
ziprasidone
Geodon
Quinolinones
Dopamine system stabilizers
aripiprazole
Abilify 
Dibenzooxepinopyrroles
asenapine
Saphris
Benzoisothiazols
lurasidone
Latuda
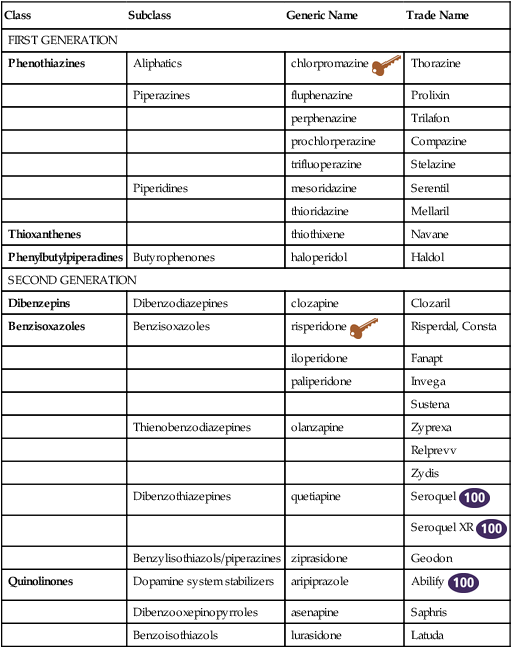
 Top 100 Icon;
Top 100 Icon;  key drug. Key drug selected because it was the first and is still in use.
key drug. Key drug selected because it was the first and is still in use.
Therapeutic Overview
Causes
Example
Metabolic and endocrine
Addison’s disease
Calcium imbalance
Carcinoid syndrome
Cushing’s syndrome
Electrolyte abnormalities
Hepatic failure
Hyperparathyroidism
Hyperthyroidism
Hypoglycemia
Hypothyroidism
Hypoxia
Magnesium imbalance
Pheochromocytoma
Porphyria
Renal failure
Serotonin syndrome
Wilson’s disease
Electrical
Complex partial seizures
Peri-ictal states (depression, hallucinations)
Postictal states (depression, dissociation, or disinhibition)
Temporal lobe status epilepticus
Neoplastic
Carcinoid syndrome
Carcinoma of the pancreas
Metastatic brain tumors
Primary brain tumor
Remote effects of carcinoma
Arterial
Arteriovenous malformations
Hypertensive lacunar state
Inflammation (cranial arteritis, lupus)
Migraine
Multi-infarct states
Subarachnoid bleeds
Subclavian steal syndrome
Thromboembolic phenomena
Transient ischemic attacks
Mechanical
Concussion
Normal pressure hydrocephalus
Subdural or epidural hematoma
Trauma
Infectious
Abscesses
AIDS
Hepatitis
Meningoencephalitis (including tuberculosis, fungal, herpes)
Multifocal leukoencephalopathy
Subacute sclerosingpanencephalitis
Syphilis
Nutritional
Vitamin B12 deficiency
Folate deficiency
Niacin deficiency
Pyridoxine (vitamin B6) deficiency
Thiamine deficiency
Degenerative and neurologic
Aging
Alzheimer’s disease
Heavy metal toxicity
Huntington’s disease
Jakob-Creutzfeldt disease
Multiple sclerosis
Parkinson’s disease
Pick’s disease
Type of Psychiatric Disorder
Examples
Chronic psychosis (severe)
Schizophrenia
Schizoaffective disorder, bipolar type (with prominent episodes of mania)
Schizoaffective disorder, depressed type (with prominent depressive episodes)
Schizophreniform (<6 months’ duration)
Chronic psychosis (less severe or bizarre)
Delusional disorder
Shared psychotic disorder
Episodic psychosis
Depression with psychotic features
Bipolar disorder (manic or depressed)
Brief psychotic disorder
PTSD; borderline personality disorder
Schizophrenia
Assessment
Mechanism of Action
Drug
Potency
D1
D2/EPS Prolactin
D4
5-HT2/Weight Gain
Anti-Cholinergic
α1/Orthostasis
α2
Histamine H1/Sedation
FIRST GENERATION
chlorpromazine (Thorazine)
Low
++
++/++
+/0
++
+/+++
+
+/+++
fluphenazine (Prolixin)
High
+
+/+++
++/0
+
+/+
+++
+/+
perphenazine (Trilafon)
Low
0
++/++
+/0
+
+/+
++
0/++
prochlorperazine (Compazine)
Low
++/+++
+
+
++
trifluoperazine (Stelazine)
High
+++
+
+
+
mesoridazine (Serentil)
0
++/+
+/0
+++
0/++
0
0/+++
thioridazine (Mellaril)
Low
+
++/+
+
+++/0
+++
+/+++
0
0/+++
thiothixene (Navane)
High
+++
+/+++
+++
+++/0
+
+/++
++
+/+
haloperidol (Haldol)
High
++
+/+++
+
+++/0
+
+/+
+++
+++/+
molindone (Moban)
0
+++/++
0
++++/0
+
+++/+
++
+++/++
loxapine (Loxitane)
High
0
+++/++
+
+/0
+
++/+
+++
+/+
SECOND GENERATION
clozapine (Clozaril)
High
+
+/+
+++
++/++++
+++/++
+/++
++
+/+++
risperidone (Risperdal)
High
++/++
++/0
0
+
++
+
iloperidone (Fanapt)
High
+
++/++
+
++/+
0
+/+
+
+
paliperidone (Invega)
High
++/++
++/+
0
+/+
+
+
olanzapine (Zyprexa)
High
+
++/+
++
+/+++
+++/++
+/++
++
+/++
quetiapine (Seroquel)
High
+++
+++/+
+++
+++/+
0/++
++/++
+++
+/++
ziprasidone (Geodon)
High
+++
+/++
+++
+
+++
+
0
++
aripiprazole (Abilify)
High
0
Partial +++/0
D3 +++
Partial 1 and 2A +++; 2c and 7 ++
+/+
+/+
+/+
asenaprine (Saphris)
High
+++
+++/+
+++
+++/+
0
+/+
++
++
lurasidone (Latuda)
High
+++/+
++/0
0
+/+
+
0 ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Antipsychotics

Only gold members can continue reading. Log In or Register to continue
