DRUG CLASSES
Cell cycle–specific agents
• Plant alkaloids
• Taxanes
• Podophyllotoxins
• Camptothecin analogs
• Antimetabolites
Cell cycle–nonspecific agents
• Alkylates
• Ethyleneimines
• Alkyl sulfonates
• Hydrazines
• Nitrosoureas
• Platinum based
• Antibiotics
PHARMACOLOGY IN PRACTICE

Patients and families undergoing treatment for a malignant disease need special consideration, understanding, and emotional support. On occasion, these needs are unrecognized by members of the health care profession. Mr. Phillip comes to the clinic for a routine blood pressure check. As he sits at your desk he becomes tearful, telling you his wife fought breast cancer only to die in a car accident. As you read about the drugs used, think about your reaction to his grief situation.
Antineoplastic drugs are one of the tools used in the treatment of malignant diseases (i.e., cancer). The term chemotherapy is often used to refer to therapy with antineoplastic drugs. Although these drugs may not always lead to a complete cure of the cancer, they often slow the rate of tumor growth and delay metastasis (spreading of the cancer to other sites). These drugs can be used for cure, control, or palliation (comfort care, the relief of symptoms at the end of life).
The Cell Cycle
All cells grow in a specific pattern of growth called the cell cycle (Fig. 50.1). During the cell cycle, different components of a cell are synthesized, and the cell divides into two new cells.
The five phases of cell growth are:
1. G1—RNA (ribonucleic acid) and proteins are built
2. S—DNA (deoxyribonucleic acid) is made from the components of the G1 phase
3. G2—RNA and protein synthesis preparing for cell division
4. M—mitotic cell division (the cell has doubled its contents and splits into two separate cells)
5. G0—the dormant or resting phase
When the cell goes into a resting phase, the cell starts performing its usual function in the body (e.g., a white blood cell might “Go” to work, fighting infection) or it prepares to start the cycle of cell division again. Some cells, such as blood cells, rapidly reproduce in a matter of hours. Other cells, such as nerve cells, complete their cell division and then go into the resting phase for years. Some cells tend to stay in the resting phase but quickly divide if the tissue is injured. Liver cells are a good example of this behavior; they do not replicate unless there is damage to the liver.
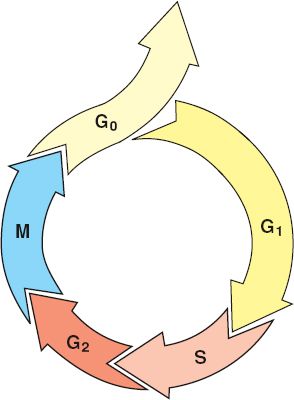
Figure 50.1 The cell cycle: G1: RNA and protein synthesis; S: DNA synthesis; G2: RNA and protein synthesis; M: mitotic cell division; G0: cell resting phase, during which the cell either differentiates to perform its function or dies.
Antineoplastic drugs are designed to attack a cell during one or many of the phases of cell division. Drugs are categorized as cell cycle specific (meaning they target the cell in one of the phases of cell division) or as cell cycle nonspecific (they can target the cell at any phase of the cycle). Many subcategories of antineoplastic drugs are available to treat malignancies. The antineoplastic drugs covered in this chapter include the cell cycle–nonspecific and cell cycle–specific drugs. Other drugs, such as biologic and chemoprotective agents, are listed in various tables. Many hormones and antihormones are used in treating cancers associated with the sex organs (see Chapter 47), and new agents that stimulate our bodies to fight cancer are increasingly becoming available (Display 50.1).
The strategy of antineoplastic drug therapy is to affect cells that rapidly divide and reproduce. Malignant neoplasms or cancerous tumors usually consist of rapidly growing (abnormal) cells. Cancer cells have no biologic feedback controls to stop their growth or proliferation. Cancer cells are more sensitive to antineoplastic drugs when the cells are in the process of growing and dividing. Chemotherapy is administered at the time the cell population is dividing as part of a strategy to optimize cell death.
Because the drugs are given systemically (i.e., they circulate through the entire body), other rapidly growing cells are usually affected by these drugs. The normal cells that line the oral cavity and gastrointestinal (GI) tract, and cells of the gonads, bone marrow, hair follicles, and lymph tissue are also rapidly dividing cells. Thus, antineoplastic drugs may affect normal as well as malignant cells, causing unpleasant adverse reactions.
Chemotherapy is administered in a series of cycles to allow for recovery of normal cells and to destroy more malignant cells (Fig. 50.2). This timing of drug administration is based on the cell kill theory principle. For example, a group of drugs are selected and this drug regimen is intended to kill about 90% of the cancer cells during the first course of treatment. This means 10% of the cancer cells still remain in the body and continue to grow. Then the second course of chemotherapy, according to this theory, targets the remaining cancer cells and reduces those cells by another 90%. Each cycle of treatment with the antineoplastic drugs kills some, but by no means all, of the cancer cells. Theoretically, when only a few cells remain, the body’s own immune system will be triggered and destroy what is left. By understanding the cell kill theory and the cell cycle, one can appreciate the rationale for using repeated doses of chemotherapy with different antineoplastic drugs. Various drugs that target cancer cells at various phases of the cell cycle are administered to kill as many cells as possible. Repeated courses of chemotherapy are used to kill an even greater proportion of the malignant cells until, theoretically, no cells are left.
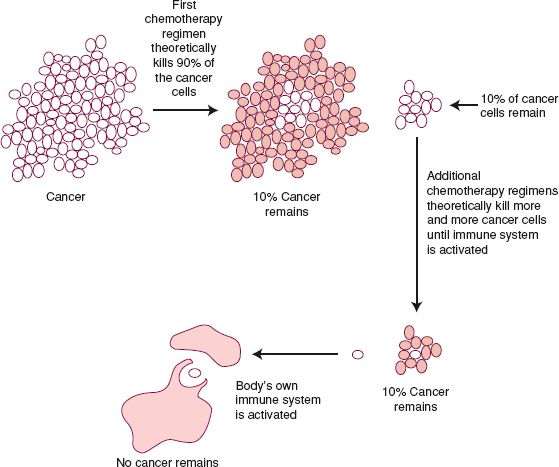
Figure 50.2 The cell kill theory: rationale for repeated chemotherapy regimens.
Display 50.1 New Frontiers in Cancer Treatment: Targeted Therapies
Used in conjunction with conventional antineoplastic drugs, targeted therapies, as the term implies, are agents used to target specific malignant cell components without hurting normal cells. Specific targeting agents include:
bexarotene (Targretin)
bortezomib (Velcade)
cetuximab (Erbitux)
crizotinib (Xalkori)
dasatinib (Sprycel)
erlotinib (Tarceva)
everolimus (Afinitor)
gefitinib (Iressa)
imatinib (Gleevec)
lapatinib (Tykerb)
nilotinib (Tasigna)
pazopanib (Votrient)
pertuzumab (Perjeta)
ruxolitinib (Jakafi)
sorafenib (Nexavar)
sunitinib (Sutent)
temsirolimus (Torisel)
tositumomab (Bexxar)
trastuzumab (Herceptin)
vandetanib (Caprelsa)
vemurafenib (Zelboraf)
vorinostat (Zolina)
Biologic Response Modifiers
aldesleukin (Proleukin)
BCG
denileukin diftitox (Ontak)
levamisole (Ergamisol)
Monoclonal Antibodies
alemtuzumab (Campath)
denosumab (Prolia)
gemtuzumab ozogamicin (Mylotarg)
ibritumomab tiuxetan (Zevalin)
ipilimumab (Yervoy)
ofatumumab (Arzerra)
panitumumab (Vectibix)
rituximab (Rituxan)
Angiogenesis Inhibitors
bevacizumab (Avastin)
interferon-alpha (Roferon-A)
lenalidomide (Revlimid)
romidepsin (Istodax)
thalidomide (Thalomid)
 HERBAL CONSIDERATIONS
HERBAL CONSIDERATIONSGreen tea and black teas come from the same plant. The difference is in the processing. Green tea is simply dried tea leaves, whereas black tea is fermented, giving it the dark color, stronger flavor, and the lowest amount of tannins and polyphenols. The beneficial effects of green tea lie in the polyphenols, or flavonoids, which have antioxidant properties. Antioxidants are thought to play a major role in preventing disease (e.g., colon cancer) and reducing the effects of aging. Green tea polyphenols are powerful antioxidants. The polyphenols are thought to act by inhibiting the reactions of free radicals in the body that are believed to play a role in aging. The benefits of green tea include an overall sense of well-being, cancer prevention, dental health, and maintenance of heart and liver health. Green tea taken as directed is safe and well tolerated. Because green tea contains caffeine, nervousness, restlessness, insomnia, and GI upset may occur. Green tea should be avoided during pregnancy because of its caffeine content. Patients with hypertension, cardiac conditions, anxiety, insomnia, diabetes, and ulcers should use green tea with caution (DerMarderosian, 2003).
CELL CYCLE–SPECIFIC DRUGS
Actions and Uses
Cell cycle–specific drugs act on the cell in one specific phase of the process of cell division, affecting both malignant and normal cells. A combination of these drugs, all acting at different phases of cell division, is typically used to treat leukemias, lymphomas, and a variety of solid tumors. The site of action of each drug depends on the drug subcategory. See the Summary Drug Table: Antineoplastic Drugs for more information.
Plant Alkaloids
Drugs that are derived from plant alkaloids include vinca alkaloids, taxanes, podophyllotoxins, and camptothecin analog drugs. The vinca alkaloids interfere with amino acid production in the S phase and formation of microtubules in the M phase. Taxanes also interfere in the M phase with microtubules. Cells are stopped during the S and G2 phases by the podophyllotoxins and thus are unable to divide. DNA synthesis during the S phase is inhibited by camptothecin analog drugs such as topotecan (Hycamtin).
Antimetabolites
Antimetabolite drugs are substances that incorporate themselves into the cellular components during the S phase of cell division. This interferes with the synthesis of RNA and DNA, making it impossible for the cancerous cell to divide into two daughter cells. These drugs are used for many of the leukemias, lymphomas, and solid tumors as well as autoimmune diseases. Methotrexate is an example of the antimetabolite drugs.
CELL CYCLE–NONSPECIFIC DRUGS
Actions and Uses
Cell cycle–nonspecific drugs interfere with the process of cell division of malignant and normal cells. Because they do not exert action specifically on one portion of the cell cycle, they are called nonspecific drugs. These drugs are used to cure, control, or provide palliation in the treatment of leukemias, lymphomas, and many different solid tumors, and are also used in the treatment of certain autoimmune diseases.
Alkylating Agents
Alkylating agents make the cell a more alkaline environment, which in turn damages the cell. Malignant cells appear to be more susceptible to the effects of alkylating drugs than normal cells. A number of subcategories are included in this group of cell cycle–nonspecific drugs. Nitrogen mustard derivatives, ethyleneimines, and platinum-based drugs all break or interfere with the crosslinks in the DNA structure. The alkyl sulfonate drug busulfan interferes with DNA of granulocytes and is used primarily for leukemias. The hydrazine group interferes with multiple phases in the synthesis of RNA, DNA, and protein. Nitrosoureas are unique in that they can cross the blood–brain barrier, and therefore are used in treating brain tumors.
Antineoplastic Antibiotics
Antineoplastic antibiotics, unlike their anti-infective antibiotic relatives, do not fight infection. Rather, their action is similar to alkylating drugs. Antineoplastic antibiotics appear to interfere with DNA and RNA synthesis, thereby delaying or inhibiting cell division and blocking the reproductive ability of malignant cells. An example of an antineoplastic antibiotic is doxorubicin, which is used in the treatment of many solid tumors.
Miscellaneous Antineoplastic Drugs
A number of drugs are used for their antineoplastic actions, but they do not belong to any one category. The mechanism of action of many of the drugs in this unrelated group is not entirely clear. Examples of miscellaneous antineoplastics are provided in the Summary Drug Table: Antineoplastic Drugs.
Adverse Reactions
Adverse reactions to antineoplastic drugs can be viewed in three different time frames: immediate (during the actual administration), during therapy cycles, and long term (many years later, during survivorship).
Immediate adverse reactions occur as a result of administration. These include nausea and vomiting from highly emetic drugs or the potential of intravenous (IV) extravasation (leakage into the surrounding tissues) of irritating solutions. Antineoplastic drugs are potentially toxic, and their administration is often associated with serious adverse reactions. At times, some of these adverse effects are allowed, because the only alternative is to stop treatment of the cancer. A treatment plan is developed that will prevent, lessen, or treat most or all of the symptoms of a specific adverse reaction. An example of prevention is giving an antiemetic before administering an antineoplastic drug known to cause severe nausea and vomiting. Display 50.2 provides a list of those drugs most likely to cause nausea and vomiting.
Display 50.2 Emetic Potential of Antineoplastic Drugs
The following drugs have a 60% or greater chance of causing nausea and vomiting when administered to patients.
Alkylating Agents
carboplatin
carmustine
cisplatin
cyclophosphamide
dacarbazine
ifosfamide
lomustine
mechlorethamine
melphalan
procarbazine
streptozocin
Antibiotics
dactinomycin
daunorubicin
doxorubicin
mitoxantrone
Antimetabolites
cytarabine
methotrexate
Plant Alkaloid
irinotecan
An example of a treatment for an adverse reaction is the administration of an antiemetic and IV fluids with electrolytes when severe vomiting is anticipated. When the drugs listed in Display 50.2 are given, antiemetic protocols should always be followed to reduce adverse reactions. Some drugs, such as platinum-based agents, may damage certain organs during administration. Again, prechemotherapy protocols for IV fluid administration are initiated to prevent adverse reactions.
Some of these reactions are dose dependent; that is, their occurrence is more common or their intensity is more severe when multiple doses (or cycles) are used. Because the antineoplastic drugs affect cancer cells and rapidly proliferating normal cells (i.e., cells in the bone marrow, GI tract, reproductive tract, and hair follicles), adverse reactions occur as the result of action on these cells.
Adverse reactions common to many of the antineoplastic drugs include bone marrow suppression (anemia, leukopenia, thrombocytopenia), stomatitis, diarrhea, and hair loss. The most common reactions are leukopenia and thrombocytopenia, which may cause cycles of chemotherapy to be delayed until blood cell counts can be raised. Some drugs, especially the alkaloids, affect the nervous system. These adverse reactions can range from a peripheral tingling sensation to hand and foot syndrome (tiny capillary leaks in extremities, causing symptoms from skin color changes to numbness).
Because the drugs used to treat cancer are effective, many people are living with the disease either cured or in remission. Some of the adverse reactions to antineoplastic drugs can have long-lasting effects. These include damage to the gonads, causing fertility problems, and to other specific organ systems, leading to cardiac, pulmonary, or neurologic problems. In addition, secondary cancers like leukemia can be caused by the original cancer treatment. These problems are listed in the Summary Drug Table: Antineoplastic Drugs. Appropriate references should be consulted when administering these drugs, because there are a variety of uses and dose ranges and, in some instances, many adverse reactions.
Contraindications and Precautions
The information discussed in this section is general, and the contraindications, precautions, and interactions for each antineoplastic drug vary. The chemotherapy nurse should consult appropriate sources before administering any antineoplastic drug.
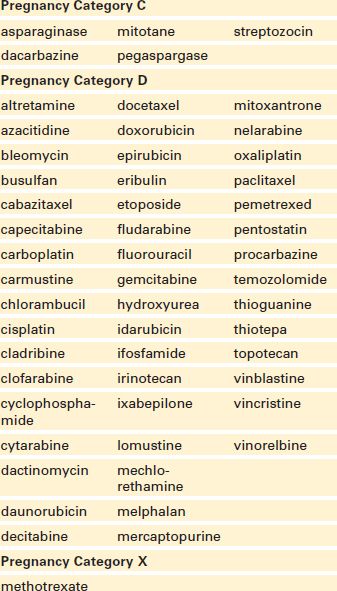
Antineoplastic drugs are contraindicated in patients with leukopenia, thrombocytopenia, anemia, serious infections, serious renal disease, or known hypersensitivity to the drug, and during pregnancy (see Display 50.3 for pregnancy classifications of selected antineoplastic drugs) or lactation.
Antineoplastic drugs are used cautiously in patients with renal or hepatic impairment, active infection, or other debilitating illnesses, or in those who have recently completed treatment with other antineoplastic drugs or radiation therapy.
Display 50.3 Pregnancy Classification for Selected Antineoplastic Drugs
Interactions
A number of antineoplastic drugs are harmful to normal cells as well as cancer cells. Cytoprotective agents are drugs used with the antineoplastic drug to protect the normal cells or organs of the body. In this way, enough of the chemotherapeutic drug can be given to eradicate the cancer without irreversible harm to the patient. Cytoprotective agents used with antineoplastic drugs are listed in Display 50.4.
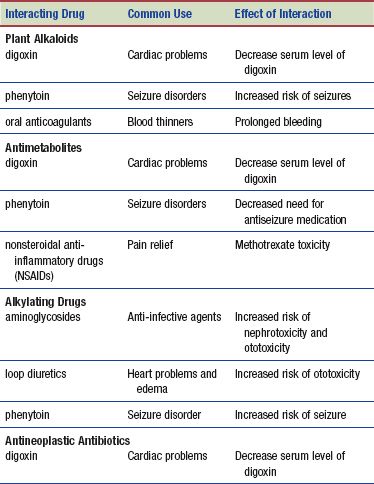
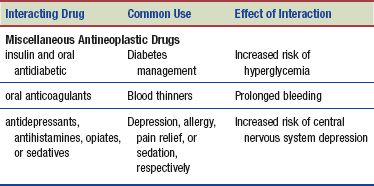
The following table lists selected interactions of the plant alkaloids, antimetabolites, alkylating drugs, antibiotics, and miscellaneous antineoplastic drugs. Typically, additive bone marrow depressive effects occur when any category of antineoplastic drug is administered with another chemotherapy drug or radiation therapy. Appropriate sources should be consulted by the chemotherapy nurse for a more complete listing of interactions before any antineoplastic drug is administered.
Display 50.4 Cytoprotective Agents
The following drugs function to protect cells or counteract adverse reactions resulting from therapeutic doses of the antineoplastic drugs.
• allopurinol, rasburicase (Elitek): Counteract the increase in uric acid and subsequent hyperuricemia resulting from the metabolic waste buildup from rapid tumor lysis (cell destruction)
• amifostine (Ethyol): Binds with metabolites of cisplatin to protect the kidneys from nephrotoxic effects, reduces xerostomia
• dexrazoxane (Zinecard): Cardioprotective agent used with doxorubicin
• leucovorin (Wellcovorin), glucarpidase (Voraxaze): Provide folic acid to cells after methotrexate administration
• mesna (Mesnex): Binds with metabolites of ifosfamide to protect the bladder from hemorrhagic cystitis
• palifermin (Kepivance): Helps epithelial cells in the oral cavity recover after severe mucositis
 HERBAL CONSIDERATIONS
HERBAL CONSIDERATIONS
The shiitake mushroom, an edible variety of mushroom, is associated with general health maintenance but not with any severe adverse reactions. Mild side effects, such as skin rashes and GI upset, have been reported. Lentinan, a derivative of the shiitake mushroom, is proving to be valuable in boosting the body’s immune system and may prolong the survival time of patients with cancer by supporting immunity. In Japan, lentinan is commonly used to treat cancer. Additional possible benefits of this herb include lowering cholesterol levels by increasing the rate at which cholesterol is excreted from the body. Under no circumstances should shiitake or lentinan be used for cancer or any serious illness without consulting a primary health care provider (DerMarderosian, 2003).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


