Chapter 29 See Chapter 28 for anatomy and physiology of the bowel. Diarrhea is categorized as acute or chronic. By definition, acute diarrhea persists for less than 2 weeks—usually, a few days to 1 week. It can be subdivided into noninflammatory or inflammatory diarrhea. Noninflammatory diarrhea is watery and nonbloody and usually is caused by a bacterium or a virus that is self-limiting. Inflammatory diarrhea consists of WBCs in the stool; these reflect invasion of the organism or toxin into the wall of the intestine (Table 29-1). TABLE 29-1 Causes of Acute Infectious Diarrhea Chronic diarrhea has an extensive number of etiologies (Table 29-2). Evaluate the patient carefully for the cause of the diarrhea, and treat the disease, not the symptom. Medications that can cause diarrhea include laxatives, antacids, magnesium-containing products, and antibiotics. TABLE 29-2 Lactose intolerance Irritable bowel disease Fecal impaction Inflammatory bowel disease Ulcerative colitis Crohn disease Microscopic colitis Malignancy Radiation Malabsorption Celiac sprue Pancreatic disease Neuropathy Chronic infection Clostridium difficile Parasites Human immunodeficiency virus (HIV)–related enteropathology
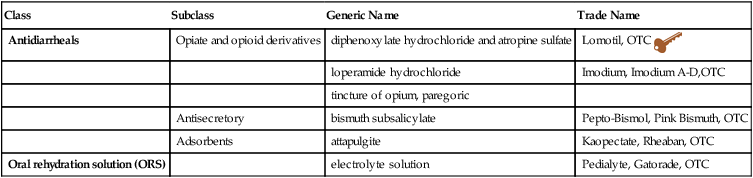
Antidiarrheals
Class
Subclass
Generic Name
Trade Name
Antidiarrheals
Opiate and opioid derivatives
diphenoxylate hydrochloride and atropine sulfate
Lomotil, OTC 
loperamide hydrochloride
Imodium, Imodium A-D,OTC
tincture of opium, paregoric
Antisecretory
bismuth subsalicylate
Pepto-Bismol, Pink Bismuth, OTC
Adsorbents
attapulgite
Kaopectate, Rheaban, OTC
Oral rehydration solution (ORS)
electrolyte solution
Pedialyte, Gatorade, OTC
Therapeutic Overview
Anatomy and Physiology
Disease Process
Cause
Noninflammatory
Inflammatory
VIRAL
Norwalk, rotavirus
Cytomegalovirus
PROTOZOAL
Giardia, Cryptosporidium
BACTERIAL
Preformed toxin
Enterotoxin production
Mucosal innervation
Staphylococcus aureus, Bacillus cereus
E. coli, Vibrio cholerae
Escherichia coli, Vibrio parahaemolyticus, Clostridium difficile, C. perfringens
Shigella, Campylobacter jejuni, Salmonella, enteroinvasive
E. coli, Chlamydia, Neisseria, Listeria
Mechanism of Action
Opioids
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

 Key drug chosen based on common usage.
Key drug chosen based on common usage. Diarrhea in pregnant women and in infants can have serious consequences, and the patient may need to be referred.
Diarrhea in pregnant women and in infants can have serious consequences, and the patient may need to be referred.
Full access? Get Clinical Tree


