Chapter 48 See Chapter 15 for discussion of diphenhydramine (Benadryl), which commonly is used off-label for sleep, particularly in geriatric patients. ∗GABA-BZ receptor agonists: nonbenzodiazepine benzodiazepine-receptor agonists. INDICATIONS • Benzodiazepines: See Table 48-1. TABLE 48-1 Indications and Unlabeled Uses of Benzodiazepines • buspirone: Generalized anxiety disorder; off-label: opiate addiction, panic attack • zolpidem: Insomnia; off-label: Parkinson’s disease • eszopiclone, zaleplon, ramelteon: Insomnia only The use of these drugs in the treatment of anxiety and insomnia is discussed in this chapter. Antidepressants have become a major category of drug treatment for anxiety. Their use in the treatment of anxiety is discussed in this chapter. See Chapter 46 for a detailed discussion of these medications. In the past, barbiturates and medications similar to barbiturates were used to treat patients with anxiety and insomnia. Newer medications seem somewhat safer with minimal drug interactions and low side effect profiles that decrease the need for barbiturates. However, they should no longer be used for these purposes because of tolerance, addiction, and seizures upon withdrawal. These agents are discussed in Chapter 45. In the primary care setting, anxiety often is a symptom of an underlying disorder, such as a medical or a psychologic problem (Box 48-1). The practitioner must obtain a comprehensive history and perform a complete physical examination of the patient to assess the possible causes and effects of the anxiety. Symptoms of anxiety vary with the subtype of anxiety experienced. The physical symptoms of anxiety are listed in Box 48-2. Elements of the history that are particularly important in evaluating anxiety include the following: • Somatic complaints that defy remedy (e.g., stomach pains, dyspnea) • Complaints of a lump in the throat • Inability to fall asleep at night—racing thoughts or worries • These symptoms may be somewhat different in children and may vary, depending on their age and other experiences with anxiety. • Five major subtypes of anxiety have been identified: generalized anxiety disorder, panic disorder, phobias, obsessive-compulsive disorder, and posttraumatic stress disorder. 1. Agoraphobia is the fear of being in a place or situation that would elicit symptoms of a panic attack and that would cause the patient to have difficulty leaving or that would cause him to be embarrassed. This often occurs in concert with a panic attack. 2. Social phobia is a fear of social situations such as public speaking. 3. Specific phobia is a fear of specific objects or situations, which may include animals, insects, heights, water, needles, and so forth.
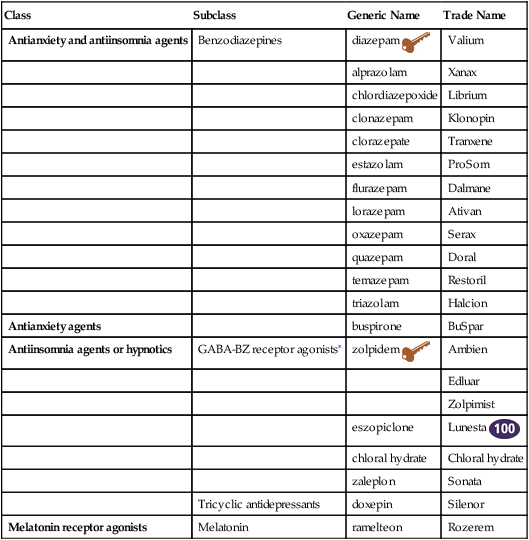
Antianxiety and Antiinsomnia Agents
Class
Subclass
Generic Name
Trade Name
Antianxiety and antiinsomnia agents
Benzodiazepines
diazepam 
Valium
alprazolam
Xanax
chlordiazepoxide
Librium
clonazepam
Klonopin
clorazepate
Tranxene
estazolam
ProSom
flurazepam
Dalmane
lorazepam
Ativan
oxazepam
Serax
quazepam
Doral
temazepam
Restoril
triazolam
Halcion
Antianxiety agents
buspirone
BuSpar
Antiinsomnia agents or hypnotics
GABA-BZ receptor agonists∗
zolpidem 
Ambien
Edluar
Zolpimist
eszopiclone
Lunesta 
chloral hydrate
Chloral hydrate
zaleplon
Sonata
Tricyclic antidepressants
doxepin
Silenor
Melatonin receptor agonists
Melatonin
ramelteon
Rozerem
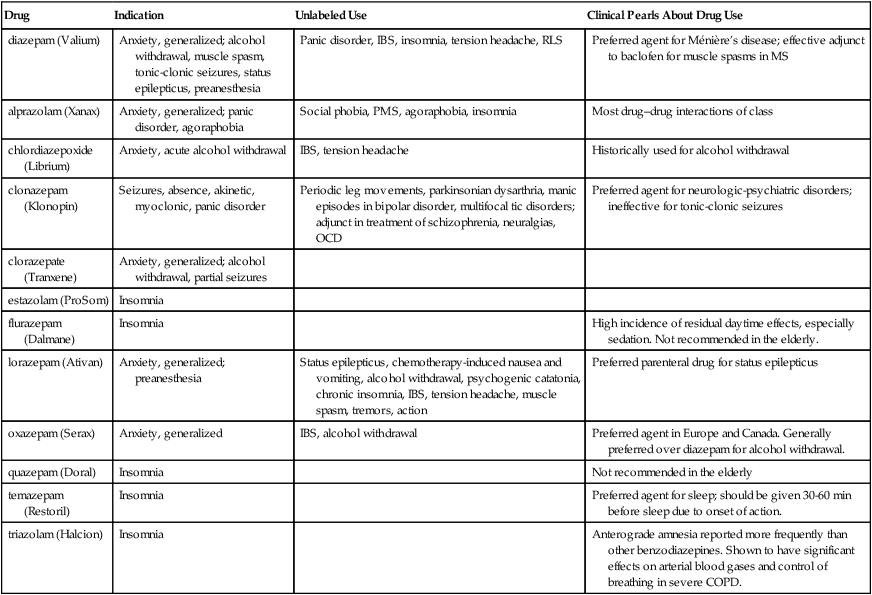
Drug
Indication
Unlabeled Use
Clinical Pearls About Drug Use
diazepam (Valium)
Anxiety, generalized; alcohol withdrawal, muscle spasm, tonic-clonic seizures, status epilepticus, preanesthesia
Panic disorder, IBS, insomnia, tension headache, RLS
Preferred agent for Ménière’s disease; effective adjunct to baclofen for muscle spasms in MS
alprazolam (Xanax)
Anxiety, generalized; panic disorder, agoraphobia
Social phobia, PMS, agoraphobia, insomnia
Most drug–drug interactions of class
chlordiazepoxide (Librium)
Anxiety, acute alcohol withdrawal
IBS, tension headache
Historically used for alcohol withdrawal
clonazepam (Klonopin)
Seizures, absence, akinetic, myoclonic, panic disorder
Periodic leg movements, parkinsonian dysarthria, manic episodes in bipolar disorder, multifocal tic disorders; adjunct in treatment of schizophrenia, neuralgias, OCD
Preferred agent for neurologic-psychiatric disorders; ineffective for tonic-clonic seizures
clorazepate (Tranxene)
Anxiety, generalized; alcohol withdrawal, partial seizures
estazolam (ProSom)
Insomnia
flurazepam (Dalmane)
Insomnia
High incidence of residual daytime effects, especially sedation. Not recommended in the elderly.
lorazepam (Ativan)
Anxiety, generalized; preanesthesia
Status epilepticus, chemotherapy-induced nausea and vomiting, alcohol withdrawal, psychogenic catatonia, chronic insomnia, IBS, tension headache, muscle spasm, tremors, action
Preferred parenteral drug for status epilepticus
oxazepam (Serax)
Anxiety, generalized
IBS, alcohol withdrawal
Preferred agent in Europe and Canada. Generally preferred over diazepam for alcohol withdrawal.
quazepam (Doral)
Insomnia
Not recommended in the elderly
temazepam (Restoril)
Insomnia
Preferred agent for sleep; should be given 30-60 min before sleep due to onset of action.
triazolam (Halcion)
Insomnia
Anterograde amnesia reported more frequently than other benzodiazepines. Shown to have significant effects on arterial blood gases and control of breathing in severe COPD.
Therapeutic Overview
Anatomy and Physiology
Disease Process
Anxiety
Phobic Disorders
Mechanism of Action
Benzodiazepines
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

 Top 100 drug;
Top 100 drug;  key drug. Diazepam is the key drug because it was the first benzodiazepine and still is in common use.
key drug. Diazepam is the key drug because it was the first benzodiazepine and still is in common use.
Full access? Get Clinical Tree


