Angiosarcoma
Key Facts
Terminology
Malignant neoplasm arising from endothelial cells or their precursors
Etiology/Pathogenesis
Breast is most common site of origin of angiosarcomas; however, they comprise < 0.1% of breast malignancies
3 groups of women who develop breast angiosarcomas
Idiopathic cases with no known cause
Women with history of breast cancer who have received radiation therapy
Women with markedly edematous arms after breast and axillary surgery for cancer (Stewart-Treves syndrome)
Clinical Issues
Idiopathic AS presents as ill-defined palpable mass in the breast
Radiation-related or edema-related AS presents with dark red or violaceous discoloration of skin
Most effective treatment is surgical removal of tumor with wide margins
Median survival: 3 years
Top Differential Diagnoses
Perilobular hemangioma
Proliferative endothelial hyperplasia
Atypical vascular lesion (AVL)
Pseudoangiomatous stromal hyperplasia (PASH)
Carcinoma
Angiolipoma
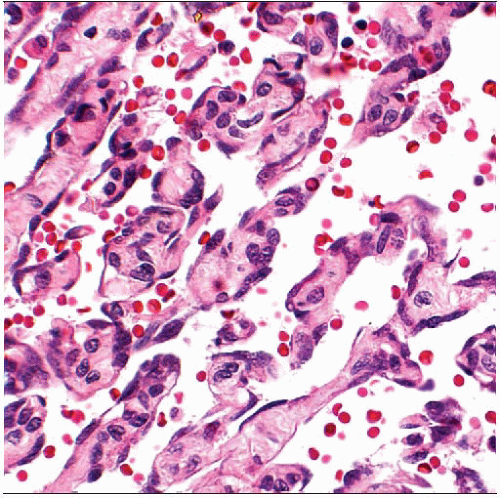 Angiosarcomas are composed of a malignant population of endothelial-type cells forming complex anastomosing channels. The lumens are filled with red blood cells. |
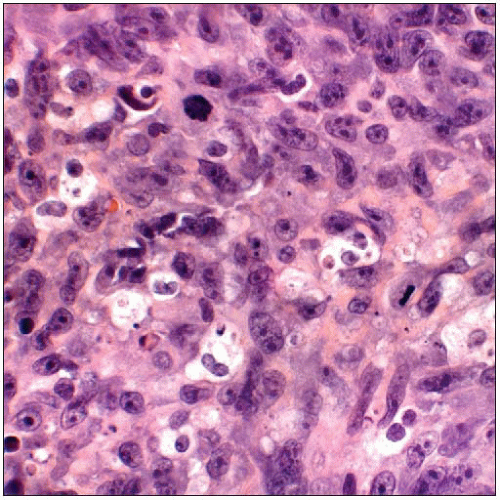 High-grade angiosarcomas can form solid sheets of epithelioid-appearing cells. Immunohistochemical studies may be necessary to distinguish recurrent carcinoma from radiation-induced angiosarcoma. |
TERMINOLOGY
Abbreviations
Angiosarcoma (AS)
Definitions
Malignant neoplasm arising from endothelial cells or their precursors
ETIOLOGY/PATHOGENESIS
Idiopathic
Breast is most common site of origin of AS
However, AS are rare tumors compared to carcinomas (< 0.1% of all breast malignancies)
Radiation
Women who have received radiation treatment for breast cancer have 9x increased risk of AS
However, absolute number of affected women is small: Approximately 3 in 1,000 women will develop AS after treatment at 15 years
Women who received chest wall radiation for Hodgkin disease are at increased risk for developing breast cancer, but AS has not been reported
Reason for this is unknown; probably related to age when radiated &&/or radiation doses
Incidence of tumors peaks from 5-10 years after treatment and is elevated out to 30 years
Edema
Women with markedly edematous arms after breast and axillary surgery for cancer are at increased risk for AS of skin (Stewart-Treves syndrome)
With more limited axillary surgery and better surgical techniques, this type of AS has become exceedingly uncommon
CLINICAL ISSUES
Epidemiology
Age
Average age of women diagnosed with idiopathic AS: 40s
Average age of women diagnosed with radiation-related or edema-related AS: 60s
Gender
Almost all patients are female; male breast AS is very rare
Site
Idiopathic AS generally arises deep in the breast
Large tumors may also involve the skin
Radiation-related AS arises in the skin
Tumors involve deeper breast tissue if large
Atypical vascular lesions (AVLs) also occur in the skin in this group of patients
Distinguishing AS from AVL may be difficult in some cases
Edema-related AS arises in the skin of edematous area
Arm is most common site
Presentation
Patients with radiation-related or edema-related AS present with dark red or violaceous discoloration of skin
Palpable mass may be associated with skin changes
Patients with idiopathic angiosarcoma present with ill-defined palpable mass in the breast
Treatment
Most effective treatment is surgical removal of tumor with wide margins
Most patients will require mastectomy to achieve this goal
Chemotherapy and radiation therapy are also used but have uncertain benefit
Prognosis
Many patients develop distant metastases
Most common sites are lung, liver, bone, and contralateral breast
Metastasis to regional lymph nodes is rare
Median survival: 3 years
Same for idiopathic and treatment-related AS
Larger tumors have poorer prognosis
Tumor grade has not been consistently linked to prognosis
IMAGE FINDINGS
Mammographic Findings
Tumors may be difficult to image as desmoplastic response commonly associated with carcinomas is not present
Ultrasonographic Findings
Tumors may appear lobulated, irregular, or ill defined
Echogenicity may be variable
May have hyperechoic areas if AS invades into adipose tissue
MACROSCOPIC FEATURES
Size
Tumors vary in size
Range: 1-20 cm
Average: 5 cm
Majority > 2 cm
Almost all vascular lesions of the breast > 2 cm in size will be malignant
Size can be difficult to determine grossly both visually and by palpation
Central portion of the tumor is usually hemorrhagic and firm to palpation
Infiltrative periphery of the tumor can blend into surrounding tissue and may not be visible
MICROSCOPIC PATHOLOGY
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


