 Chapter 5 Abdomen and Pelvis
Chapter 5 Abdomen and Pelvis
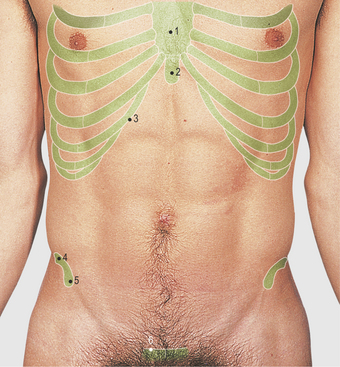
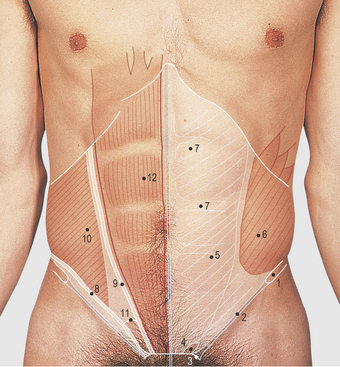
Anterior abdominal wall (Figs 5.1–5.8)
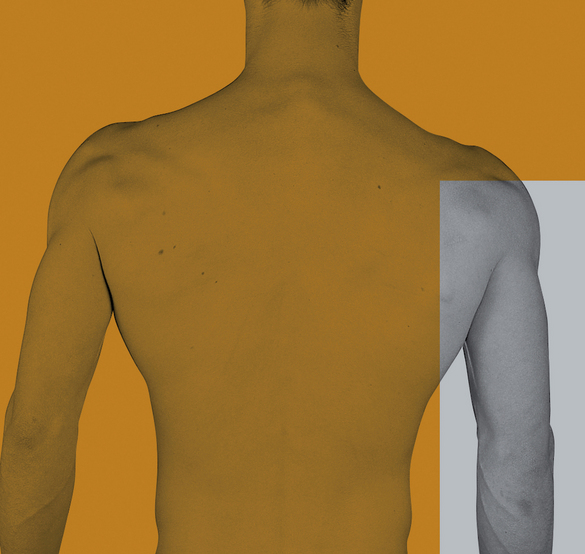
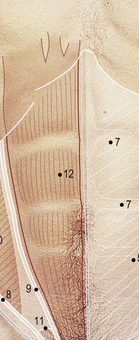
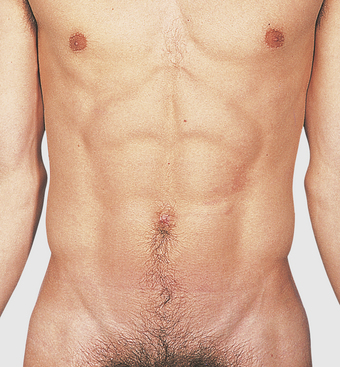
The anterior abdominal wall is bounded superiorly by the lower costal margin and inferiorly by the symphysis pubis, the pubic crest and tubercle, the inguinal ligament, the anterior superior iliac spine and the iliac crest, from medial to lateral (Fig. 5.2). The wall comprises three flat sheet-like muscles. They fuse medially to form a fibrous sheath for the vertically running rectus abdominis muscles, lying on each side of the midline. The sheaths of the two sides meet in the midline as a fibrous raphe, known as the linea alba. The three transverse lines of attachment of the rectus abdominis muscle to the anterior sheath can be seen in a muscular subject above the umbilicus; they are termed tendinous intersections (Fig. 5.1). The superior end of the rectus abdominis muscle crosses the anterior rib cage to be attached to the fifth, sixth and seventh costal cartilages from lateral to medial. The lateral line of formation of the rectus sheath is known as the linea semilunaris.
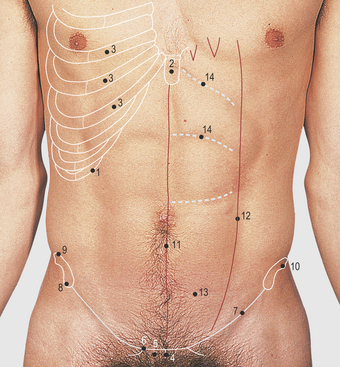
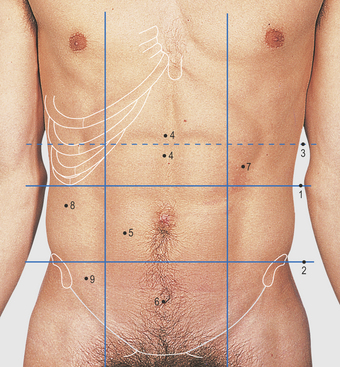
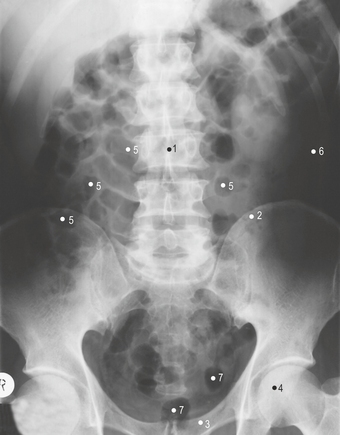
The anterior abdominal wall is divided for descriptive purposes into nine regions by two horizontal lines (subcostal and transtubercular) and two vertical lines through the midpoint of each clavicle (Fig. 5.5 – these lines cross the costal margin at the tip of the ninth costal cartilage and the midinguinal point). The subcostal plane passes through the lower border of the third lumbar vertebra; the transtubercular plane passes through the iliac tubercle and the fifth lumbar spine. The three central regions formed by these lines are the epigastrium, umbilical and suprapubic, from above downwards. The three regions on each side are the hypochondrium, lumbar and iliac, from above downwards. Another plane sometimes referred to in clinical practice is the horizontal, transduodenal (transpyloric) plane, passing through the first part of the duodenum. It is at the level of the lower border of the first lumbar vertebra; ventrally, the transpyloric plane lies midway between the xiphisternal joint and the umbilicus. The abdominal cavity extends upwards behind the lower ribs under the diaphragm and downwards into the pelvis to the pelvic diaphragm (formed by the levator ani muscles).
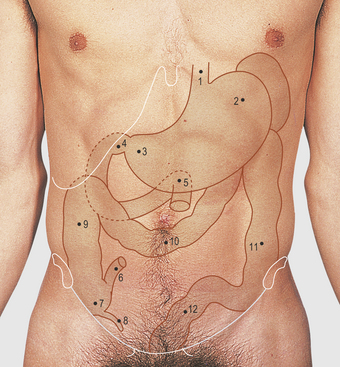
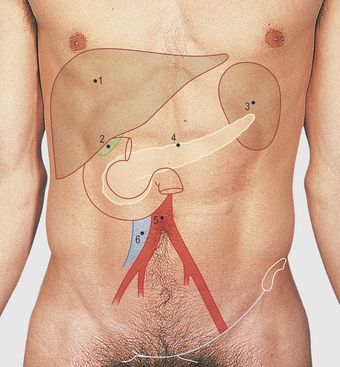
Surface markings of the alimentary tract (Fig. 5.6)
The base of the appendix is sited in the right iliac fossa. The surface marking is approximately at the junction of the middle and lateral thirds of a line joining the umbilicus to the anterior superior iliac spine. Initially, inflammation of the appendix produces referred pain around the umbilicus (i.e. the 10th thoracic dermatome) but, as it progresses and involves the parietal peritoneum, local tenderness becomes more marked in the right iliac fossa. The tip of the appendix is usually positioned laterally, inferior to, or behind the caecum, but it may pass downwards into the pelvis or be related to the terminal ileum. The caecum, ascending colon and hepatic flexure of the colon on the right side, and the splenic flexure descending colon on the left, are largely retroperitoneal structures whereas the transverse and sigmoid colons have a mesentery and vary in their position, although they are usually in the regions shown (Fig. 5.6).



