http://evolve.elsevier.com/McCuistion/pharmacology
This chapter discusses two groups of drugs that affect the sympathetic nervous system—adrenergic agonists, or sympathomimetics, and adrenergic antagonists, also called adrenergic blockers or sympatholytics—along with their dosages and uses.
 Patient Safety
Patient SafetyIntravenous (IV) adrenergic agonists and antagonists are high-alert medications because they can cause significant harm to a patient in the event of a medication error.
Adrenergic Agonists
Drugs that stimulate the sympathetic nervous system are called adrenergic agonists, adrenergics, or sympathomimetics because they mimic the sympathetic neurotransmitters norepinephrine and epinephrine. They act on one or more adrenergic receptor sites located in the effector cells of muscles such as the heart, bronchiole walls, gastrointestinal (GI) tract, urinary bladder, and ciliary muscles of the eye. There are many adrenergic receptors. The four main receptors are alpha1, alpha2, beta1, and beta2, which mediate the major responses described in Table 15.1 and illustrated in Fig. 15.1.
The alpha-adrenergic receptors are located in the blood vessels, eyes, bladder, and prostate. When the alpha1 receptors in vascular tissues (vessels) of muscles are stimulated, the arterioles and venules constrict; this increases peripheral resistance and blood return to the heart, circulation improves, and blood pressure is increased. When too much stimulation occurs, blood flow is decreased to the vital organs.
The alpha2 receptors are located in the postganglionic sympathetic nerve endings. When stimulated, they inhibit the release of norepinephrine, which leads to a decrease in vasoconstriction. This results in vasodilation and a decrease in blood pressure.
TABLE 15.1
Effects of Adrenergic Agonists at Receptors
| Receptor | Physiologic Responses |
| Alpha1 | Increases force of heart contraction; vasoconstriction increases blood pressure; mydriasis (dilation of pupils) occurs; secretion in salivary glands decreases; urinary bladder relaxation and urinary sphincter contraction increases |
| Alpha2 | Inhibits release of norepinephrine; dilates blood vessels; produces hypotension; decreases gastrointestinal motility and tone |
| Beta1 | Increases heart rate and force of contraction; increases renin secretion, which increases blood pressure |
| Beta2 | Dilates bronchioles; promotes gastrointestinal and uterine relaxation; promotes increase in blood glucose through glycogenolysis in the liver; increases blood flow in skeletal muscles |
The beta1 receptors are located primarily in the heart but are also found in the kidney. Stimulation of the beta1 receptors increases myocardial contractility and heart rate.
The beta2 receptors are found mostly in the smooth muscles of the lung and GI tract, the liver, and the uterine muscle. Stimulation of the beta2 receptor causes (1) relaxation of the smooth muscles of the lungs, which results in bronchodilation; (2) a decrease in GI tone and motility; (3) activation of glycogenolysis in the liver and increased blood glucose; and (4) relaxation of the uterine muscle, which results in a decrease in uterine contraction (Fig. 15.2; see also Table 15.1).
Other adrenergic receptors are dopaminergic and are located in the renal, mesenteric, coronary, and cerebral arteries. When these receptors are stimulated, the vessels dilate and blood flow increases. Only dopamine can activate these receptors.
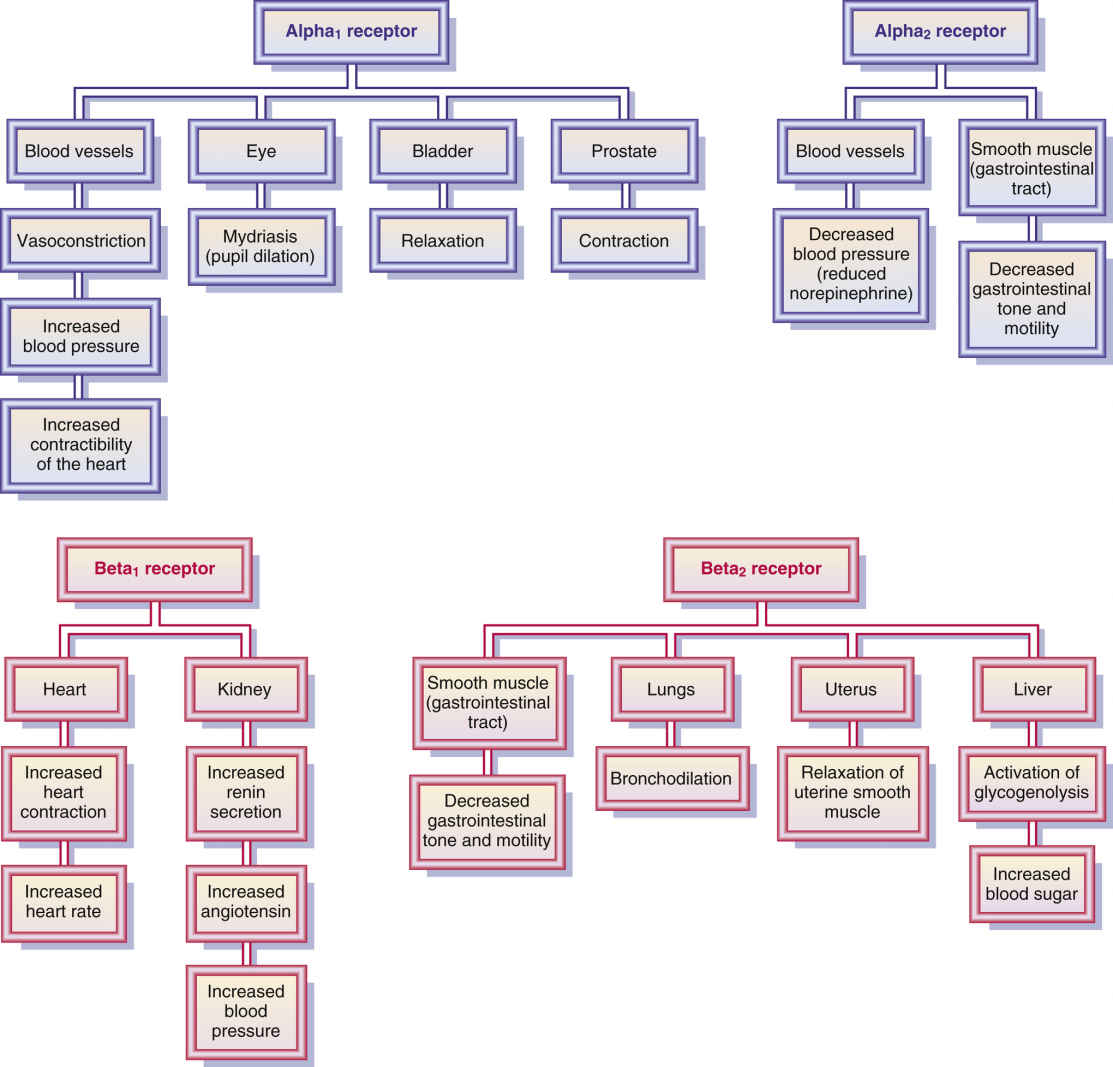
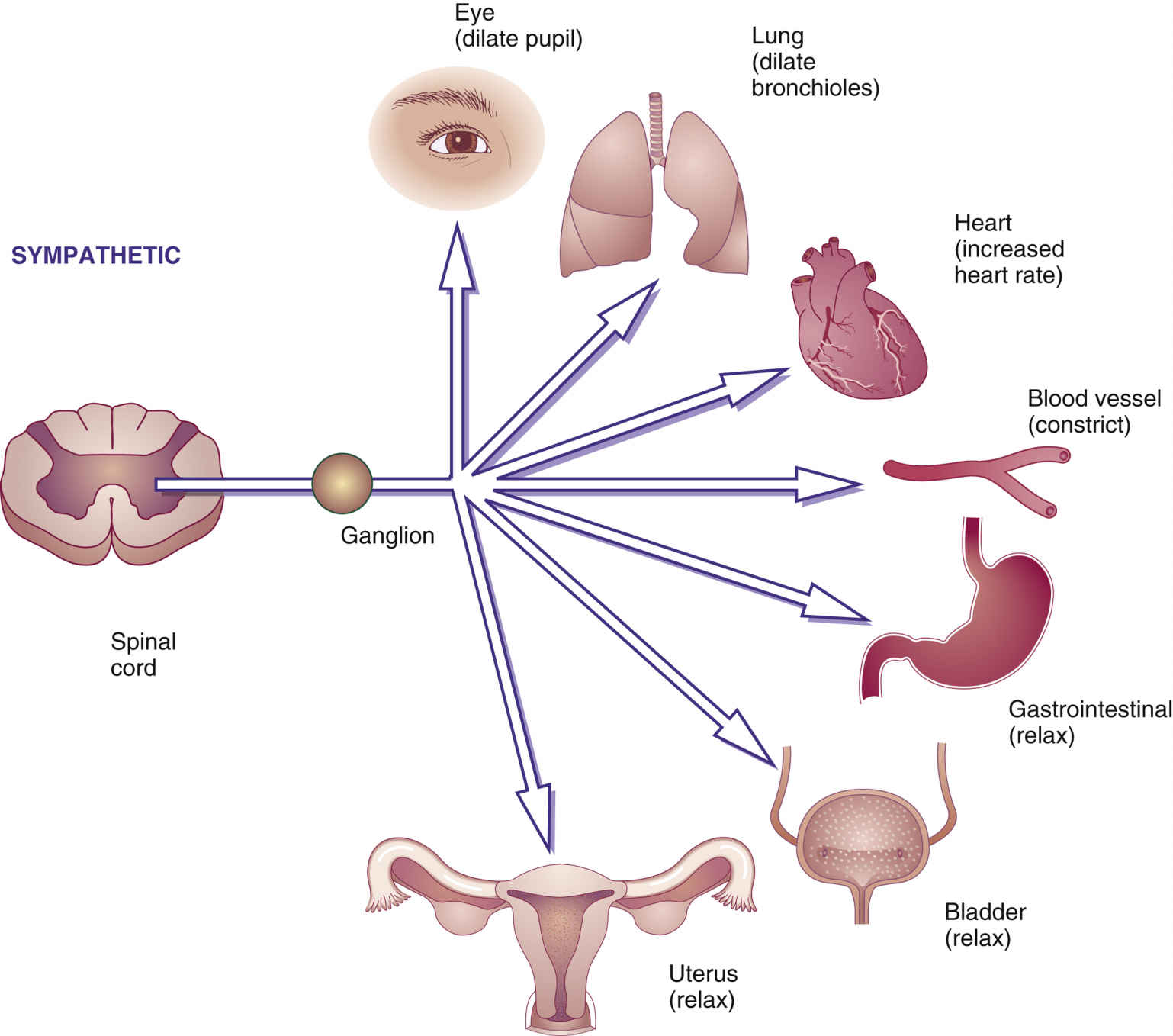
FIG. 15.2 Sympathetic responses. Stimulation of the sympathetic nervous system or use of sympathomimetic (adrenergic agonist) drugs can cause the pupils and bronchioles to dilate; heart rate to increase; blood vessels to constrict; and muscles of the gastrointestinal tract, bladder, and uterus to relax, thereby decreasing contractions.
Inactivation of Neurotransmitters
After the neurotransmitter (e.g., norepinephrine) has performed its function, the action must be stopped to prevent prolonging the effect. Transmitters are inactivated by (1) reuptake of the transmitter back into the neuron (nerve cell terminal), (2) enzymatic transformation or degradation, and (3) diffusion away from the receptor. The mechanism of norepinephrine reuptake plays a more important role in inactivation than does the enzymatic action. Following the reuptake of the transmitter in the neuron, the transmitter may be degraded or reused. The two enzymes that inactivate norepinephrine are monoamine oxidase (MAO), which is inside the neuron, and catechol-O-methyltransferase (COMT), which is outside the neuron.
Drugs can prolong the action of the neurotransmitter (e.g., norepinephrine) by either inhibiting reuptake, which prolongs the action of the transmitter, or inhibiting the degradation by enzymatic action.
Classification of Sympathomimetics
The sympathomimetic (adrenergic agonist) drugs that stimulate adrenergic receptors are classified into three categories according to their effects on organ cells. Categories include (1) direct-acting sympathomimetics, which directly stimulate the adrenergic receptor (e.g., epinephrine or norepinephrine); (2) indirect-acting sympathomimetics, which stimulate the release of norepinephrine from the terminal nerve endings (e.g., amphetamine); and (3) mixed-acting (both direct- and indirect-acting) sympathomimetics, which stimulate the adrenergic receptor sites and stimulate the release of norepinephrine from the terminal nerve endings (e.g., ephedrine, Fig. 15.3).
Pseudoephedrine is an example of a mixed-acting sympathomimetic: It acts indirectly by stimulating the release of norepinephrine from the nerve terminals, and it acts directly on the alpha1 and beta1 receptors. Pseudoephedrine, like epinephrine, increases heart rate. It is not as potent a vasoconstrictor as epinephrine, and the risk of hemorrhagic stroke and hypertensive crisis is less. Pseudoephedrine is helpful to relieve nasal and sinus congestion without rebound congestion.
Catecholamines are the chemical structures of a substance, either endogenous or synthetic, that can produce a sympathomimetic response. Examples of endogenous catecholamines are epinephrine, norepinephrine, and dopamine. The synthetic catecholamines are isoproterenol and dobutamine. Noncatecholamines such as phenylephrine, metaproterenol, and albuterol stimulate the adrenergic receptors. Most noncatecholamines have a longer duration of action than the endogenous or synthetic catecholamines.
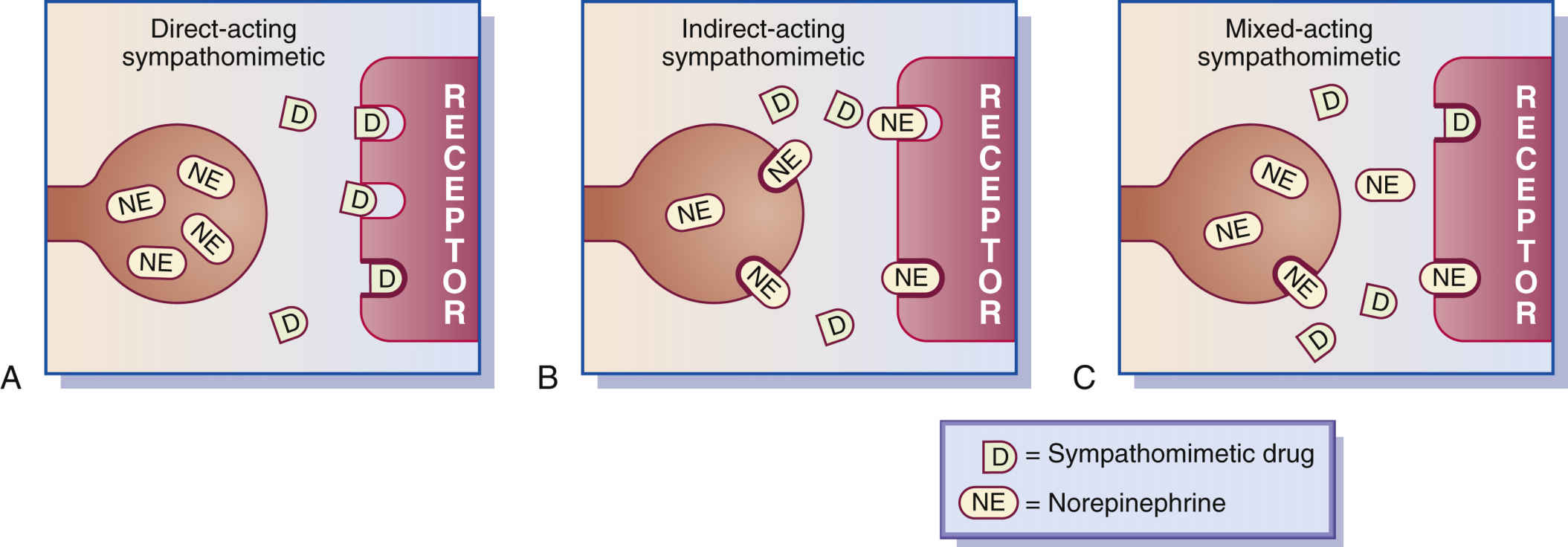
FIG. 15.3 A, Direct-acting sympathomimetics. B, Indirect-acting sympathomimetics. C, Mixed-acting sympathomimetics.
Many of the adrenergic agonists stimulate more than one of the adrenergic receptor sites. An example is epinephrine, which acts on alpha1-, beta1-, and beta2-adrenergic receptor sites. The responses from these receptor sites include increase in blood pressure, pupil dilation, increase in heart rate (tachycardia), and bronchodilation. In anaphylactic shock, epinephrine is useful because it increases blood pressure, heart rate, and airflow through the lungs. Because epinephrine affects different adrenergic receptors, it is nonselective. Additional side effects result when more responses occur than are desired. Pseudoephedrine is commonly used for illegal production of amphetamine and methamphetamine. National regulatory measures control pseudoephedrine drug sales with individual limits of 3.6 g/day and 9 g within 30 days. Identifications are scanned with each purchase. The database is linked nationally and keeps a 2-year tally. Prototype Drug Chart 15.1 lists the pharmacologic behavior of epinephrine.
Epinephrine
Pharmacokinetics
Epinephrine can be administered subcutaneously, intravascularly (vastus lateralis), intravenously, topically, by inhalation, or via intracardiac administration. It is not given orally because it is rapidly metabolized in the GI tract and liver, which results in unstable serum levels. The half-life of epinephrine and the percentage by which the drug is protein bound are unknown. Epinephrine is metabolized by the liver and is excreted in the urine.
Pharmacodynamics
Epinephrine is frequently used in emergencies to treat anaphylaxis, a life-threatening allergic response. Epinephrine is a potent inotropic (myocardial contraction–strengthening) drug that increases cardiac output, promotes vasoconstriction and systolic blood pressure elevation, increases heart rate, and produces bronchodilation. High doses can result in cardiac dysrhythmia, which necessitates electrocardiogram (ECG) monitoring. Epinephrine can also cause renal vasoconstriction, thereby decreasing renal perfusion and urinary output.
The onset of action and peak concentration times are rapid. The use of decongestants with epinephrine has an additive effect. When epinephrine is administered with digoxin, cardiac dysrhythmia may occur. Beta blockers can antagonize the action of epinephrine. Tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs) allow epinephrine’s effects to be intensified and prolonged.


Side Effects and Adverse Reactions
Undesired side effects frequently result when the adrenergic drug dosage is increased or when the drug is nonselective. Side effects commonly associated with adrenergic agonists include hypertension, tachycardia, palpitations, restlessness, tremors, dysrhythmia, dizziness, urinary retention, nausea, vomiting, dyspnea, and pulmonary edema.
Names of adrenergic drugs, the receptors they activate, dosage information, and common uses are listed in Table 15.2. Epinephrine is also discussed in Chapter 55 as one of the drugs used during emergencies.
Albuterol
Albuterol sulfate, a beta2-adrenergic agonist, is selective for beta2-adrenergic receptors, so the response is relaxation of bronchial smooth muscle and bronchodilation. A patient with asthma may tolerate albuterol better than isoproterenol, which activates beta1 and beta2 receptors, because albuterol’s action is more selective; it activates only the beta2 receptors of smooth muscle in the lungs and uterus and in the vasculature that supplies the skeletal muscles. By using selective sympathomimetics, fewer undesired adverse effects will occur. However, high dosages of albuterol may affect beta1 receptors, causing an increase in heart rate. Prototype Drug Chart 15.2 lists the drug data related to albuterol.
Pharmacokinetics
Albuterol sulfate is well absorbed from the GI tract and is extensively metabolized by the liver. The half-life of albuterol via oral inhalation is 2.7 to 6 hours.
Pharmacodynamics
The primary use of albuterol is to prevent and treat bronchospasm. With inhalation, the onset of action of albuterol is 5 to 15 minutes by inhalation, and the duration of action is 2 to 6 hours.
Side Effects and Adverse Reactions
Tremors, restlessness, and nervousness are the most common side effects of oral or inhalation albuterol. If albuterol is taken with an MAOI, a hypertensive crisis can result. Other side effects include tachycardia, palpitations, dizziness, dysrhythmia, nausea, vomiting, and urinary retention. Beta antagonists (beta blockers) may inhibit the action of albuterol. Albuterol and the beta2 drugs are also discussed in Chapters 36 and 39, respectively.
 Nursing Process: Patient-Centered Collaborative Care
Nursing Process: Patient-Centered Collaborative CareAdrenergic Agonists
Assessment
• Record baseline vital signs for future comparisons.
• Assess the patient’s drug history.
• Determine patient’s health history. Most adrenergic agonists are contraindicated if the patient has a cardiac dysrhythmia, narrow-angle glaucoma, or cardiogenic shock.
• Determine baseline glucose level.
Nursing Diagnoses
• Sleep Pattern, Disturbed related to the adverse drug effect of insomnia
• Knowledge, Deficient related to drug administration
Planning
• Patient’s vital signs will be within acceptable ranges.
• Patient will experience therapeutic effects by improved blood pressure, breathing pattern, and cardiac output.
Nursing Interventions
• Administer IV epinephrine 1 mg (10 mL of a 1:10,000 concentration per American Heart Association [AHA] guidelines) for cardiac resuscitation; may repeat every 3 to 5 minutes. Follow each dose with a 20-mL saline flush to ensure proper delivery. Normally, epinephrine is administered 1 mg IV over 1 minute or more.
•  Monitor IV site frequently when administering norepinephrine bitartrate or dopamine because extravasation of these drugs causes tissue damage and necrosis within 12 hours. These drugs should be diluted sufficiently in IV fluids.
Monitor IV site frequently when administering norepinephrine bitartrate or dopamine because extravasation of these drugs causes tissue damage and necrosis within 12 hours. These drugs should be diluted sufficiently in IV fluids.
Monitor IV site frequently when administering norepinephrine bitartrate or dopamine because extravasation of these drugs causes tissue damage and necrosis within 12 hours. These drugs should be diluted sufficiently in IV fluids.• Administer antidote, phentolamine mesylate, 5 to 10 mg, diluted in 10 to 15 mL of normal saline infiltrated into the area for IV extravasation of norepinephrine and dopamine.
• Record patient’s vital signs. Report signs of increasing blood pressure and increasing heart rate. If the patient receives an alpha-adrenergic agonist intravenously for shock, check the blood pressure every 3 to 5 minutes or as indicated to avoid severe hypertension.
• Monitor ECG for dysrhythmia when adrenergic agonists are given intravenously.
• Report side effects of adrenergic drugs such as tachycardia, palpitations, tremors, dizziness, and increased blood pressure.
• Check patient’s urinary output and assess for bladder distension. Urinary retention can result from a high drug dose or continuous use of adrenergic agonists.
• Offer food to the patient when giving adrenergic agonists to avoid nausea and vomiting.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


