What is the embryonic origin of the adrenal medulla?
The adrenal medulla arises from ectoderm derived from the neural crest.
Adrenal Medulla
•Originates from ectoderm
•Produces epinephrine (20%) and norepinephrine (80%)
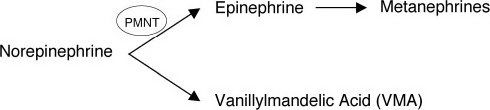
What are the only two locations where epinephrine is produced in the human body, and why is this?
The enzyme responsible for converting norepinephrine to epinephrine is phenylethanolamine-N-methyltransferase. This particular enzyme is located in only two areas of the human body: The adrenal medulla and the Organ of Zuckerkandl (sympathetic paraganglia near the aortic bifurcation).
A 38-year-old female has an abdominal CT scan to evaluate her pelvic and lower abdominal pain. The CT demonstrates an ovarian cyst and a 2.5-cm left adrenal mass. What is the next step in management?
The adrenal mass is an adrenal incidentaloma. Given its small size, it does not account for the patient’s symptoms and it can be further evaluated on an elective basis. Furthermore, any evaluation of an adrenal mass requires a work-up to answer the following three important questions:
1. Is it functioning or non-functioning?
2. Is it benign or malignant?
3. Is it primary or secondary?
Considerations in Evaluating an Adrenal Mass
1.Functioning (Metabolically Active) vs. Non-functioning
•The vast majority of adrenal masses are non-functioning
•Hyperfunctioning lesions should generally be resected, regardless of size
•A diagnosis of a hyperfunctioning gland is made by history, physical exam, and blood and urine levels of primary and secondary metabolites (catecholamines, metanephrines, vanillylmandelic acid [VMA])
•The degree of autonomous function can be measured and can aid in diagnosis (adrenal hyperplasia vs. adrenal adenoma vs. adrenal carcinoma)
•Hyperplasia is sensitive to negative feedback with inhibition of secretion
•Adenoma is intermediately sensitive to negative feedback
•Carcinoma is usually autonomous
2.Benign vs. Malignant
•The vast majority of adrenal masses are benign
•Hyperplastic mass
•Adenoma
•Benign cyst
•Carcinomas are rare and approximately 50% have metastases at the time of diagnosis
•CT assists in diagnosis
3.Primary vs. Secondary
•Secondary (metastatic) lesions originate from lung, breast, renal cell, melanoma, prostate, and colon cancers
•In fact, metastasis to the adrenal gland is the most common cause of an adrenal mass if the patient has a history of malignancy
A colonoscopy, as well as a breast and pelvic or prostate exam should be performed in all patients with a suspicious adrenal, hepatic, or atypical intra-abdominal mass.
Adrenal Incidentalomas
•Defined as an adrenal mass discovered during abdominal imaging performed for an unrelated reason
•Most are small, benign, non-functioning cortical adenomas (and have no clinical significance)
•The prevalence of “serendipitous” masses is reported to be 1% to 2% of CT scans (similar to autopsy studies)
•The differential diagnosis includes cortical adenoma (most common), adrenocortical carcinoma (rare), pheochromocytoma, ganglioneuroma, cyst, organized hemorrhage or fibrosis, and metastasis
An incidentaloma is most commonly an adrenal adenoma.
Studies to Evaluate an Adrenal Mass
•Serum electrolytes (hypercortisolism may present as hypokalemia and hypernatremia)
•24-hour urine cortisol
•Plasma cortisol, estradiol, testosterone, dehydroepiandrosterone, and androstenedione
•A low-dose (1 mg) dexamethasone cortisol suppression test
•Normally, this should suppress pituitary ACTH resulting in a decrease in measured urinary cortisol levels
•If there is no suppression, suspect Cushing disease
•Then follow-up with a high-dose dexamethasone suppression test to diagnose an autonomously functioning adrenal tumor
•Serum renin-to-aldosterone ratio
•Urinary catecholamines, metanephrines, VMA
•Serum 17-OH steroids and 17-ketosteroids
The best diagnostic screening test for Cushing syndrome is a low-dose overnight dexamethasone suppression test.
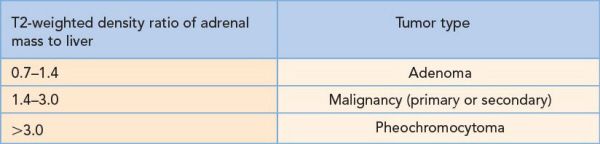
CT Scan Characteristics of Adrenal Masses
•Benign tumors are usually round/oval, smooth, and homogenous
•Adenomas contain increased fat content and thus have a low density
•Malignant tumors are irregular and non-homogeneous from focal hemorrhage and necrosis
•A cyst can be identified and further evaluation may include aspiration with cytology
•Positive (malignant) cytology, evidence of hormonal activity, and recurrence after needle aspiration are indications for surgical resection
•Homogeneous fatty lesions (myelolipoma and lipomas) may be diagnosed by CT scan and generally require no further investigation or treatment regardless of size
Resect adrenal masses that are hyperfunctioning, large (>4 to 6 cm), growing, or have suspicious characteristics on CT scan (irregular borders/heterogeneity).
Magnetic Resonance Imaging Characteristics
•Contraindicated if there is an indication for surgery—a general surgical principle true to many types of suspicious masses in the body
•May be performed when multiple masses are present and a primary diagnosis is unknown based on other tests
•May be of particular value in a patient with a known extra-adrenal malignancy
•It is not helpful in differentiating adrenal adenoma from adrenal cortical carcinoma (as with most neuroendocrine tumors in the body)
•Not appropriate for a hormonally active tumor, larger tumors, or if pheochromocytoma is even remotely suspected—all of which are surgical indications
Do not perform percutaneous needle biopsy on an adrenal mass until it is confirmed that the lesion is non-functional.
A 64-year-old man is found to have a 3.5-cm adrenal mass and hypertension. His urinary catecholamines are noted to be markedly elevated. Is surgical resection indicated?
While this patient does not meet criteria for resection based on adrenal size alone, the presence of biologic activity (i.e., hyperfunction) is an indication for surgical resection. Other criteria for surgical resection include malignancy and size.
Indications for Surgery
•Hyperfunction
•Increased aldosterone (Conn syndrome)
•Increased cortisol (Cushing syndrome)
•Increased catecholamines (pheochromocytoma)
•Malignancy
•CT findings may indicate the presence of a malignancy
•Size >4 to 6 cm
•For non-functioning masses <4 cm, DO NOT OPERATE
•Follow size and character with CT at regular intervals (e.g., 3, 6, 12 months, and yearly)
•Resect if there is an increase in size or if it becomes metabolically active (i.e., hyperfunctioning)
•For non-functioning masses 4 to 6 cm, INDIVIDUALIZE
•May resect or observe (consider Magnetic resonance imaging [MRI])
•In younger patients (<40 years), in whom adenomas are less common, consider surgery
•In elderly patients with significant comorbidity and operative risk, consider not operating, since the natural history of such intermediate size incidentalomas is still poorly understood
•Resect if the mass becomes metabolically active
•For non-functioning masses >6 cm, OPERATE
•Resect because of increased risk of malignancy
•Begin a metastatic work-up for cancer
•The only contraindications to resection are
•Adrenal metastasis
•Other metastatic disease
•An asymptomatic, well-characterized lipoma or myelolipoma
A 47-year-old woman with refractory hypertension on three antihypertensive medications is noted on routine blood-work to be hypokalemic. A CT scan is obtained. What is the most likely diagnosis?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


