• Positive: CK-PAN, CK7, CK19, CEA-M, CA19-9, MUC1, and MUC5AC
CK20, CDX-2 positive in < 50% of cases
Top Differential Diagnoses
• Reactive periductal glands
• Pancreatic ductal carcinoma: Indistinguishable histologically and immunophenotypically
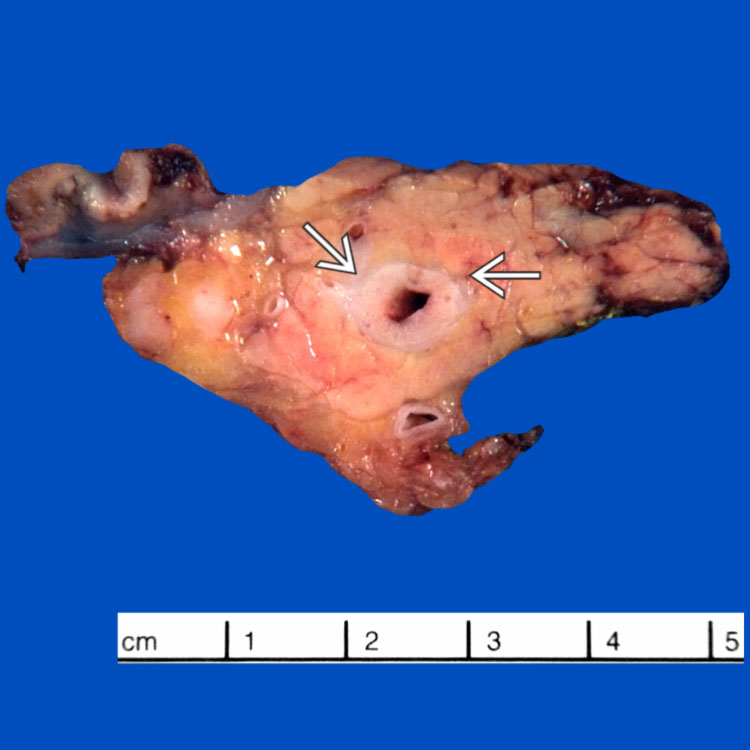
Gross Appearance This cross section from a Whipple resection shows distal bile duct carcinoma involving the intrapancreatic portion of the common bile duct. Note the marked thickening of the duct wall .
Widely Spaced Irregular Glands This case of extrahepatic cholangiocarcinoma features widely spaced, irregular glands infiltrating the duct wall. The duct lumen is partially denuded . Note the presence of residual benign periductal glands arranged in a lobular pattern .
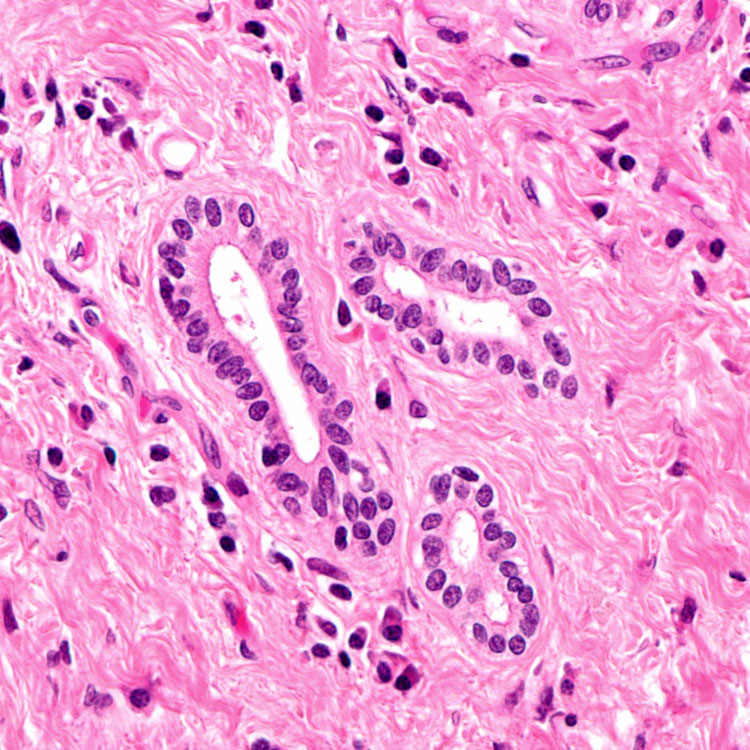
High-Power View These tumors are often very well differentiated, such as this case featuring well-formed glandular structures lined by a single layer of cuboidal epithelial cells with minimal cytologic atypia.
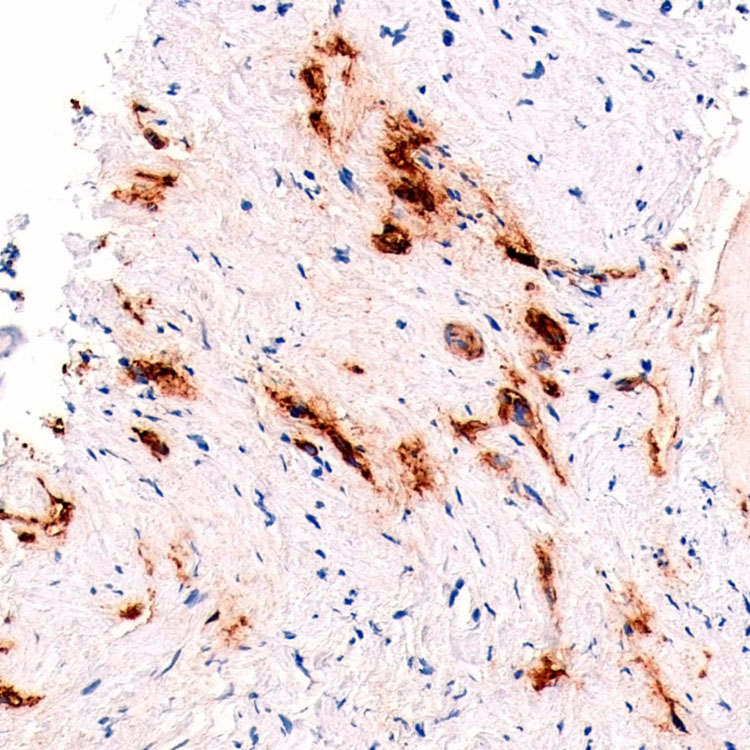
CK7 An extrahepatic bile duct biopsy shows poorly differentiated adenocarcinoma with cord-like clusters and individual cells infiltrating desmoplastic stroma. The tumor cells are immunoreactive with CK7.
TERMINOLOGY
Synonyms
• Extrahepatic cholangiocarcinoma
Definitions
• Malignant biliary epithelial neoplasm arising from right or left hepatic duct, common hepatic duct, or common bile duct
• Perihilar: Arises in extrahepatic bile ducts upstream from origin of cystic duct (70-80%)
Klatskin tumor: Perihilar tumor occurring at confluence of right and left hepatic ducts
• Distal: Arises in common bile duct, including intrapancreatic portion, above ampulla of Vater (20-30%)



 .
.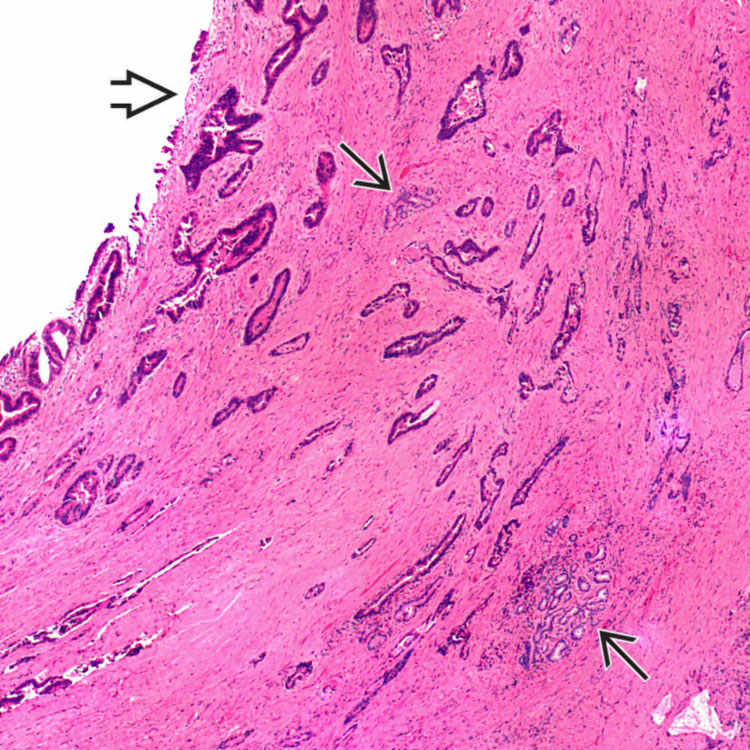
 . Note the presence of residual benign periductal glands arranged in a lobular pattern
. Note the presence of residual benign periductal glands arranged in a lobular pattern  .
.