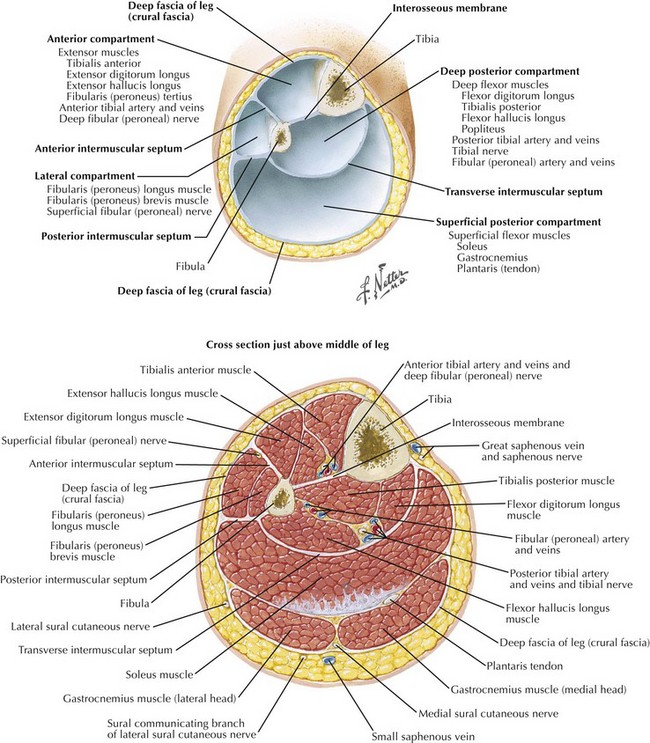
Chapter 39 Use of immediate postoperative prosthesis (IPOP) typically is surgeon and institution specific. IPOP allows for early weight bearing and ambulation and is well suited for younger, motivated patients. The goal of operation is to provide a healed wound with a stump that can fit into a prosthetic limb. For BKA, the long posterior myocutaneous flap is typically used, although circular and fish-mouth incisions may be necessary with wounds in or on the calf. Newer prosthetic techniques allow for mediolateral or anteroposterior flaps with good functional outcome. The importance of identifying the fascial layers for closure and meticulous handling of the tissues should be emphasized (Fig. 39-1).
Above-Knee and Below-Knee Amputation
Surgical Principles
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine