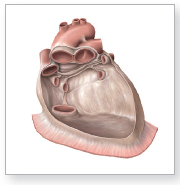
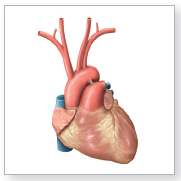
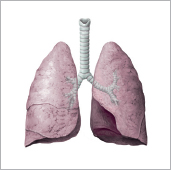
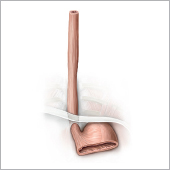
23.1 Thymus Location • Situated in the mediastinum superius posterior to the sternum, and anterior to the pericardium and major vessels at the basis cordis • Projection on the thorax is referred to as the thymic triangle. Shape and structure • Lymphoepithelial organ, usually consists of two lobi (left and right lobes). • Delicate connective tissue capsule, and trabeculae that extend into the parenchyma subdividing the thymus into lobuli • Each lobulus is divided into a (darker) cortex and (lighter) medulla. Epithelial cells form a densely packed subcapsular layer around the fibrous trabeculae (blood–thymus barrier) and join together inside the thymus to form a three-dimensional network that encloses the lymphocytes. Epithelial cells in the medulla aggregate to form Hassall’s corpuscles. • Other cell types: macrophages, myoid cells, dendritic cells Neurovascular structures (see also p. 400) Mediastinal circulation. Owing to its location in the mediastinum superius, the thymus is supplied by the neurovascular structures of the mediastinum (entering and exiting the head). • Arteries: rr. thymici arising from the a. thoracica interna (proximity to sternum); • Veins: vv. thymicae drain into the vv. brachiocephalicae. • Lymphatic drainage: through the nll. brachiocephalici into the trunci bronchomediastinales • Autonomic innervation: – parasympathetic through both nn. vagi, especially the nn. laryngei recurrentes – sympathetic through branches of the ganglia cervicalia (nn. cardiaci cervicales) Function • Maturation and differentiation (conferring immunological competence) of T-cells • Induction of programmed cell death (apoptosis) in T-cells that respond to antigens: approximately 90 % of immature T-cells die in the thymus. • Production of immune-modulating hormones (thymosin, thymopoietin, thymulin) • Primary lymphatic organ Note: The thymus is an organ “of childhood and adolescence.” It reaches its maximum size during puberty (approximately 30 grams). The degree of atrophy of thymic tissue in adults varies. Embryonic development • The thymic epithelium is derived from the epithelium of the saccus pharyngeus tertius (endodermal origin). • The epithelial primordium is populated with lymphocytes (mesodermal origin). Major diseases • Disorders of the thymus are very rare • Absence of the thymus may be life-threatening (thymic aplasia), resulting in lack of cellular immunity • Lymphatic diseases (e.g., certain types of leukemia) may affect the thymus • Thymomas: tumors that originate from the epithelial cells of the thymus, and because of the immunologic function of the thymus are often accompanied by autoimmune diseases: myasthenia gravis (muscle weakness). Location Situated in the thorax (mediastinum medium) Shape and structure Fibrous sac that surrounds the cor consisting of • Pericardium fibrosum (outermost layer composed of dense connective tissue; extends to the roots of the great vessels at the basis cordis); • Pericardium serosum (serous membrane) with – lamina parietalis (adhered to the pericardium fibrosum), – lamina visceralis (epicardium, attached to the myocardium); • Between laminae parietalis and visceralis: cavitas pericardiaca (narrow space); • At the location where the lamina visceralis is folded back onto the lamina parietalis near the basis cordis, two sinuses are formed: – sinus transversus pericardii (between the arteries and veins) – sinus obliquus pericardii (between the vv. pulmonales sinistrae and dextrae). Openings • One for the aorta ascendens • One for the truncus pulmonalis • Two for both vv. cavae • Four for the four vv. pulmonales. Neurovascular structures (see also p. 403) • Mediastinal circulation • Arteries: a. pericardiacophrenica (from the a. thoracica interna) • Veins: v. pericardiacophrenica (to the v. brachiocephalica) • Lymphatic drainage: nll. prepericardiaci, nll. pericardiaci laterales (also nll. phrenici superiores and nll. tracheobronchiales into the truncus bronchomediastinalis) • Autonomic innervation: negligible • Somatosensory innervation: n. phrenicus (from the plexus cervicalis) Function Provides sliding-surface for the heart, however the pericardium is not essential for life. Embryonic development Derived from mesoderma laminae lateralis: • Visceral parts derived from mesenchyma splanchnopleurale • Parietal parts derived from mesenchyma somatopleurale Major diseases • Pericarditis: inflammation usually caused by viral or bacterial infection. • Tuberculous pericarditis, which is rare nowadays, can lead to pericardial calcium deposits. As a result, the heart can no longer expand; it is constricted (also known as constrictive pericarditis). Location • Located in the thorax within the pericardium. • The basis cordis is directed upward, backward, and to the right. The basis cordis is the location of the venous entry and arterial exit points (vv. cavae inferior and superior, vv. pulmonales, aorta ascendens and truncus pulmonalis). • The apex cordis is directed downward, forward and to the left. • The longitudinal axis of the cor (from the base to the apex, the anatomical axis of the cor) is at a 45-degree angle to all body planes. Shape and structure • Hollow organ, shaped like a cone: measures 12–14 cm in length, 9 cm in width at its broadest part. • Weight: up to 300 g. External structures of the cor • Surfaces: – facies sternocostalis (facies anterior) – facies pulmonales dextra and sinistra – facies diaphragmatica (facies inferior) • Grooves on the outside of the cor: – sulci interventriculares anterior/posterior – sulcus coronarius • Auriculae atrii: (auricula sinistra/dextra): protrusions attached to the atria (analogous to the primitive atria; potential site for thrombus formation) produce atrial natriuretic peptide (ANP) for regulation of blood pressure. Internal structures of the cor Chambers and openings of the cor • Four contractile chambers: – two atria: atria sinistrum and dextrum separated by the septum interatriale (muscle); – two ventriculi: ventriculi sinister and dexter, separated by the septum interventriculare (pars muscularis and pars membranacea, thus part muscle and part connective tissue); both ventriculi have an inflow tract (with trabeculae carneae) and an outflow tract (smooth-walled) following the direction of blood flow. • Four openings that connect the atria and ventriculi, the ventriculus dexter and truncus pulmonalis, and the ventriculus sinister and aorta ascendens: – two openings in the right side of the cor: ostium atrioventriculare dextrum and ostium trunci pulmonalis; – two openings in the left side of the cor: ostium atrioventriculare sinistrum and ostium aortae. • Additionally, openings for the two vv. cavae (in the atrium dextrum) and the four vv. pulmonales (in the atrium sinistrum, see flow of blood below) as well as the ostium sinus coronarii (in the atrium dextrum: opening of sinus coronarius with the valvula sinus coronarii). Flow of blood through the heart chambers • Generally: from the right cor to the lungs (oxygen absorption), from there to the left cor and then to the aorta (oxygen is released to serially connected organs) • More specifically: from the vv. cavae superior and inferior into the atrium dextrum, from there through the ostium atrioventriculare dextrum to the ventriculus dexter and through the ostium trunci pulmonalis to the truncus pulmonalis, through both of the aa. pulmonales, and into the lungs; from there to the four vv. pulmonales, then to the atrium sinistrum and through the ostium atrioventriculare sinistrum to the ventriculus sinister and finally through the ostium aortae to the aorta. Cardiac valves • By closing and opening (mm. papillares, see below) four valves ensure that blood flows in only one direction through the cor: – two valvae atrioventriculares; – two semilunar valves (valva trunci pulmonalis and valva aortae). During ventricular contraction, the valvae atrioventriculares prevent backflow of blood from the ventriculi into the atria; when the ventriculi relax, the semilunar valves prevent the return of blood from the truncus pulmonalis and aorta ascendens back into the ventricles. • Valves of the right side of the cor: – valva atrioventricularis dextra at the ostium atrioventriculare dextrum = cuspid valve with three cusps: cuspides septalis/anterior/posterior = tricuspid valve; – valva trunci pulmonalis at the ostium trunci pulmonalis in the outflow tract of the ventriculus dexter = semilunar valve with three cusps: valvula semilunares anterior/sinistra/dextra; • Valves of the left side of the cor: – valva atrioventricularis sinistra at the ostium atrioventriculare sinistrum = cuspid valve with two cusps = bicuspid valve: cuspides anterior/posterior = valva mitralis; – valva aortae at the ostium aortae in the outflow tract of the ventriculus sinister = semilunar valve also with three cusps: valvulae semilunares posterior/sinistra/dextra. Grooves and crests on the inner walls of the chambers of the cor Grooves (only in the atria): • Right: fossa ovalis in the septum interatriale is the embryonic remnant of the foramen ovale. • Left: valvula foraminis ovalis is the counterpart of the fossa ovalis on the right side. Crests (in atria and ventriculi): • Atria dextrum and sinistrum: mm. pectinati: ridge-like muscle protrusions in the auricula, see above, correspond to the primitive atrium of the embryonic cor. • Ventriculi dexter and sinister: – trabeculae carneae (muscular columns that line the ventriculi; more prominent in the ventriculus dexter than in the ventriculus sinister) – mm. papillares: specialized extensions of the trabeculae carneae that project into the lumen of the ventriculus; prevent the inversion or prolapse of valves during ventricular contraction – in the ventriculus dexter: three mm. papillares for the three cusps of the valva tricuspidalis, see above, (anterior, posterior, and septalis) – in the ventriculus sinister: two mm. papillares for the two cusps of the bicuspid valve (valva mitralis), see above (mm. papillares anterior and posterior) Skeleton of the cor The heart valves all lie in one plane (valve plane) and are covered by endocardium. The valve rings are composed of dense connective tissue. All anuli fibrosi, together with the collagenous bands through which they are connected, form the cardiac skeleton. Layers of the heart wall The wall of the cor consists of three layers. From the inside to the outside they are • endocardium (simple squamous epithelium): lines the cavities of the cor and covers the heart valves; • myocardium (muscle, the fibers of which are arranged in different directions): muscle fibers roughly arranged in three layers; • epicardium (tunica serosa of the pericardium, simple squamous epithelium): strictly speaking, it is part of the pericardium, although it is often referred to as part of the cor. Neurovascular structures (see also p. 402) • Mediastinal circulation • Arteries: a. coronaria sinistra (with r. interventricularis anterior and r. circumflexus) and a. coronaria dextra (with r. interventricularis posterior), both arise from the aorta ascendens where it exits the ventriculus sinister. • Veins: vv. cardiacae (magna, media, parva), like the v. ventriculi sinistri posterior, the vv. cardiacae return blood to the atrium dextrum through the sinus coronarius. • Lymphatic drainage: through the nll. brachiocephalici and the nll. tracheobronchiales into the truncus bronchomediastinalis • Autonomic innervation: parasympathetic through the two nn. vagi (rr. cardiaci cervicales and thoracici). The neuronal cell bodies are in the nuclei posteriores nervorum vagorum; sympathetic through branches of ganglia thoracica 2–5 (nn. cardiaci cervicales superior, medius and inferior) and rr. cardiaci thoracici. Function The cor functions as a suction-pressure pump to distribute blood around the body (heart volume approximately 780 ml, ventricular stroke volume 70 ml). • The heartbeat can be felt as pulse (resting heart rate ~1 Hz). • Cardiac activity is divided into two phases: systole (contraction of the myocardium) and diastole (relaxation of the myocardium). • Contraction of the ventricular myocardium (closure of the AV valves) and closure of the valvae aortae and trunci pulmonalis are audible as the first and second heart sounds. • Cardiac excitation conduction system composed of specialized myocardial cells: impulses are generated by the nodus sinuatrialis (SA node) in the atrium dextrum adjacent to the opening of the v. cava superior. Excitation is spread to the ventriculi through the nodus atrioventricularis (AV node), at the junction of atrium dextrum and ventriculus dexter, and then through the fasciculus atrioventricularis (bundle of His) with its crura dextrum and sinistrum, which terminate in the Purkinje fibers. Note: Because of its autonomous excitation, the cor can trigger the impulse that generates the heartbeat. Even an isolated heart beats. The autonomic innervation (see above) modifies only the activities of the autonomous excitation and conduction system. The parasympathetic nervous system reduces the heart rate and atrioventricular conduction. The sympathetic nervous system increases both as well as the stroke volume. Embryonic Development Of mesodermal origin, derived from the primitive cor tubulare and subsequently formed ansa cordis. Major diseases • Heart diseases are important and are the leading cause of death in the industrialized world: myocardial infarction = occluded aa. coronariae that lead to inadequate blood flow to distinct parts of the myocardium, which results in myocardial necrosis • Arrhythmia and dysfunction of the conduction system • Valve defects (congenital or caused by inflammation of the endocardium) = incomplete opening of the valve (valve stenosis) or incomplete valve closure (valve insufficiency) • With myocardial injuries without damage to the pericardium, the cor continues to pump blood into the cavitas pericardiaca until cardiac arrest occurs (cardiac tamponade). • Generally: formation of pathological blood clots (thromboses) in the cor, which may travel through the blood stream, for example, to the encephalon. Location • Pars cervicalis of the trachea situated in the neck • Pars thoracica of the trachea and bronchi principales situated in the mediastinum • Bronchi lobares and all segments inferior: intrapulmonary location • Lungs: situated on either side of the mediastinum • Surface of the lung covered by pleura visceralis (pleura pulmonalis). On the facies mediastinalis at the lig. pulmonale the pleura parietalis is folded back onto the pleura visceralis. External structure of the lung • Apex pulmonis • Basis pulmonis • Lobi pulmonis. Three lobi in the right lung: lobus superior, lobus medius, and lobus inferior; two in the left lung: lobus superior and lobus inferior • Fissures, two in the right lung: fissura horizontalis below the lobus superior; fissura obliqua between the lobus medius and lobus inferior. In the left lung one fissura obliqua between the lobi superior and inferior • Two margines: margines anterior and inferior • Four surfaces: facies costalis (adjacent to the ribs), facies diaphragmatica (at the basis pulmonis, adjacent to the diaphragma), facies mediastinalis (adjacent to the mediastinum), facies interlobaris (in the fissurae between lobi) Note: A term for the posterior margin of the lung (where the facies costalis and mediastinalis meet) is not listed in the official Terminologia Anatomica. Shape and structure of the airways • Generally: tubes that divide by dichotomous branching with decreasing caliber • The intrapulmonary airways, connective tissue, and neurovascular structures form a spongy organ—the paired pulmones. Structure of the trachea and arbor bronchialis: • Trachea to bronchioli terminales = conducting (carrying air) portion. • Bronchioli terminales to alveoli = respiratory (gas exchange) portion. Components of the conducting portion: • Pars cervicalis of the trachea: first tracheal ring, see below, to apertura thoracis superior • Pars thoracica of the trachea: apertura thoracis superior to bifurcatio tracheae • At the bifurcatio tracheae: division of the trachea into the bronchi principales dexter and bronchi principales dexter • Division of the bronchus principalis dexter into three bronchi lobares: bronchi lobares superior dexter, medius and inferior dexter • Division of the bronchus principalis sinister into two bronchi lobares: bronchi lobares superior sinister and inferior sinister • Division of the bronchi lobares into bronchi segmentales: ten bronchi segmentales in the right lung and nine bronchi segmentales in the left lung • Division of the bronchi segmentales into bronchi intrasegmentales Components of the respiratory portion: • Bronchioli respiratorii: first to third order (where alveoli begin to appear) • Ductuli alveolares • Sacculi alveolares Structure of the airway wall Trachea: • Hollow, tubular organ with 16–20 horseshoe-shaped cartilage rings • Tracheal rings joined together by collagen and elastic fibers (ligg. anularia) • Tunica mucosa of the trachea covered with respiratory epithelium, contains multiple glands (gll. tracheales). • Posterior tracheal wall: non-cartilaginous, composed of connective tissue (membranous wall of trachea), permeated by smooth-muscle cells (m. trachealis). Bronchi principales, lobares, segmentales and intrasegmentales: • Generally similar in structure to the trachea. • Concentric or spiral sheets of smooth-muscle cells in all bronchi (active changes in caliber) • In bronchi segmentales and intrasegmentales cartilaginous plates instead of cartilage rings • Pseudostratified respiratory epithelium like tracheal mucosa Starting from the bronchioli respiratorii: • Non-cartilaginous walls • Ciliated epithelium with type I and type II pneumocytes (in the alveoli) Internal structure of the lungs Structure of the airways determines the structure of the pulmones: • Both lungs aerated by trachea. • Bronchi principales (sinister and dexter, respectively) each aerate one lung (sinister and dexter, respectively). • Bronchi lobales each aerate one lobus. • Bronchi segmentales each aerate one segmentum bronchopulmonale. • Bronchioli terminales each aerate one lobulus (pulmonary lobule). • Bronchioli respiratorii each aerate one acinus; a group of acini forms a lobulus. Neurovascular structures (see also p. 404) Mediastinal circulation • The intrapulmonary neurovascular structures in the lung either run along the divisions of the arbor bronchialis or within the connective tissue framework. • Characteristic feature of the lungs: two circulation systems: rr. bronchiales (aortae) and vv. bronchiales to supply the lung itself, and aa. and vv. pulmonales for gas exchange through the entire body. Bronchial arteries and veins: • Arteries: rr. bronchiales directly from the aorta thoracica or indirectly from aa. intercostales posteriores • Veins: on the right, vv. bronchiales to the v. azygos, on the left to the v. hemiazygos or v. hemiazygos accessoria Arteriae and venae pulmonales: • Arteries: the aa. pulmonales (sinistra, dextra) carry deoxygenated blood from the truncus pulmonalis. Segmental branches (aa. segmentales) of the aa. pulmonales follow the bronchi segmentales into the center of one of the 10 or 9 segmenta bronchopulmonalia. • Veins: drainage of oxygenated blood usually through four vv. pulmonales into the atrium sinistrum of the cor • Lymphatic drainage: through the nll. intrapulmonales, bronchopulmonales, tracheobronchiales, and paratracheales into the trunci bronchomediastinales • Autonomic innervation: – parasympathetic through the two nn. vagi to the plexus pulmonalis, – sympathetic through branches mainly from ganglia thoracica 2 or 3–4 (varies), also to the plexus pulmonalis Function Generally, the exchange of oxygen and carbon dioxide between the atmosphere and blood circulation, more specifically: • Trachea and bronchi as well as their divisions (arbor bronchialis) except for the finest terminal portions: air conduction • Final divisions of the arbor bronchialis (alveoli): gas exchange between atmosphere and blood; thus the important role of the lungs for – energy production: oxygen is extracted from the atmosphere for oxidation processes. – regulation of acid-base balance (release of carbon dioxide in the air when exhaling and thus influencing bicarbonate levels in the blood) • Following changes in the thoracic volume through the pleural layers (capillary forces cause the pleura visceralis, which is attached to the lungs, to adhere to the pleura parietalis, which is attached to the inner surface of the thoracic wall); a change in lung volume leads to a change in intrapulmonary pressure resulting in drawing in or expelling air from the lungs. Embryonic development Of endodermal origin, derived from the cranial praeenteron: • Gemma respiratoria or diverticulum laryngotracheale develops from a small outpouching on the ventral surface of the embryonic oesophagus. • Gemma respiratoria undergoes repeated dichotomous branching (total of 22) to give rise to the trachea along with the arbor bronchialis including the alveoli. Note: The lungs are fully matured at approximately the age of 10. Major diseases The arbor bronchialis and lungs are the parts of the body most commonly affected by diseases (entry points for infectious pathogens): • Acute inflammation of the arbor bronchialis (bronchitis, bronchial catarrh, cold) is usually caused by viral infections and is generally harmless. • Chronic inflammation (chronic bronchitis) is much more common in smokers. • Bronchial asthma (often triggered by allergies) is a result of insufficient expansion of small bronchi and bronchioli during expiration. • Lung overexpansion and rupture of the alveoli (pulmonary emphysema) • Chronic obstructive pulmonary disease (COPD): endstage of the three previously mentioned diseases, with destruction of gas exchange tissue • Malignant tumors (bronchial carcinoma) is among the leading causes of death for smokers. • Pulmonary embolism: Acute occlusion of an a. pulmonalis (or one of its branches) is caused by a blood clot that most commonly was formed in a vein and carried from the right cor to the lung. In that case it is crucial that the pulmones possess a double circulation. Blood from the bronchial branches is sufficient to supply the tissue. Hence, blockage of the a. pulmonalis does not result in tissue undersupply and subsequent destruction. Location Situated in the neck and thorax (mediastinum) between the trachea and columna vertebralis, as well as in the abdomen Shape, size and segments • Tubular organ, measures about 23–27 cm in length from the entrance of the oesophagus to its terminal portion. • Measures about 20 mm in width (but see constrictions of the oesophagus). Divided into three parts corresponding to the regions of the body they are located in (see above) • Pars cervicalis (C 6–T 1): to the apertura thoracis superior • Pars thoracica (T 1–T 11): to the hiatus oesophageus (site where the oesophagus passes through the diaphragma) • Pars abdominalis: to the ostium cardiacum of the gaster (shortest segment, measures only 2–3 cm in length, lies intraperitoneally). Esophageal constrictions (maximum width of 14 mm instead of the usual 20 mm) • Upper constriction: constrictio pharyngooesophagealis at the C6 level; 14–16 cm from the dentes incisivi • Middle constriction: constrictio partis thoracicae at the T 4/T 5 level; 25–27 cm from the dentes incisivi, oesophagus passes to the right of the aorta thoracica. • Lower constriction: constrictio phrenica at the T 10/T 11 level; 36–38 cm from the dentes incisivi, site where the oesophagus pierces the diaphragma; functional closure of the esophagus by muscles and venous cushions of the oesophageal wall, and muscles of the diaphragma Wall structure • Basically the same as in the gastrointestinal tract: tunica mucosa, tela submucosa, tunica muscularis, and tunica adventitia, or in the lower part in proximity to the gaster: tela subserosa and tunica serosa. • Tunica mucosa with stratified non-keratinized squamous epithelium (has no digestive function but provides mechanical protection against passing food, lubricated by gll. oesophageae) • Musculature in the upper oesophagus (variable degree of expansion), striated (like the mm. pharyngis), in the middle and lower part smooth muscle (like the gaster), the lower part contains numerous veins. • Muscles also contain fibers that wind obliquely around the oesophagus. • Combination of circular and longitudinal muscle fibers allows for the expansion and constriction of the oesophageal inlet and outlet (swallowing). Neurovascular structures (see also p. 401) • Primarily mediastinal circulation (pars thoracica); to a lesser extent also cervical (pars cervicalis) and upper abdominal circulation (pars abdominalis) • Arteries: numerous rr. oesophageales of the a. thyroidea inferior (pars cervicalis), aorta thoracica (pars thoracica), and a. gastrica sinistra (pars abdominalis) • Veins: numerous vv. oesophageales to the v. thyroidea inferior (pars cervicalis), vv. azygos and hemiazygos (pars thoracica), and v. gastrica sinistra (pars abdominalis) • Lymphatic drainage through the nll. juxtaoesophageales into the nll. cervicales profundi (pars cervicalis), trunci bronchomediastinales (pars thoracica) and nll. gastrici sinistri (pars abdominalis) • Autonomic innervation: – parasympathetic through the two nn. vagi (trunci vagales), in the neck region specifically through the nn. laryngei recurrentes. Neurons for the smooth esophageal muscles in the nucleus posterior nervi vagi, neurons for the striated muscles in nucleus ambiguus – sympathetic through branches of ganglia thoracica 2–5. The autonomic fibers form the plexus oesophageus on the oesophagus. Function During swallowing, active transport of solids and liquids from the pharynx to the gaster; when vomiting, transport of gaster contents from the gaster to the pharynx Embryonic development • Derived from the endoderm of the cranial praeenteron. • Lower part of the mesoesophagus may remain in the form of the lig. hepatoesophageale (connects hepar to pars abdominalis of oesophagus). Note: As a result of the rotation of the gaster in the embryo, the oesophagus also shifts slightly. Thus, the longitudinal layer of the smooth esophageal muscles is arranged in a rightward spiral pattern. Major diseases Diseases of the oesophagus itself (rare except for esophageal reflux): • Diverticulum (outpouchings of the wall), most common at the junction between the hypopharynx (pars laryngea pharyngis) and oesophagus (also known as Zenker’s diverticulum, which is not an esophageal but a hypopharyngeal diverticulum). • Malignant tumors (esophageal carcinoma; relatively rare) • Inflammation of the tunica mucosa oesophagi as a result of chronic alcohol consumption • Esophageal reflux: inflammation of the esophageal epithelium caused by reflux of stomach acid; caused by insufficient closing mechanisms at the junction of the oesophagus and gaster. • Barrett’s oesophagus: as a result of chronic esophageal reflux, the columnar epithelium of the gaster may replace the squamous epithelium of the oesophagus: increased risk of cancer. In the case of liver cirrhosis, abnormally enlarged esophageal veins (esophageal varices: hemorrhagic risk) serve as a portacaval detour (drainage into the azygos system!). Location Lies intraperitoneally in the left upper quadrant (=epigastrium). Shape and segments • Sac-like hollow organ with parietes anterior and posterior; different shapes may be encountered (hook-shaped gaster, bull-horn-shaped gaster, long gaster). • Four parts of the gaster in cranial to caudal direction: – top right: cardia = ostium cardiacum = esophageal inlet – fundus gastricus (base or dome of the gaster; appears on radiographs as an air-filled space above a fluid level) – corpus gastricum – bottom right: pars pylorica of gaster = pylorus with antrum pyloricum and canalis pyloricus; stomach terminates at the pylorus, which closes the ostium pyloricum (exit from the gaster into the duodenum) • The corpus gastricum has two curvaturae: – curvatura minor, faces right and upward, omentum minus (connects the hepar to the gaster) extends from it. – curvatura major, faces left and downward, omentum majus extends from it. • The gaster has two notches: – the incisura cardialis at the junction between the cardia and the corpus gastricum – the incisura angularis at the junction between the corpus gastricum and the pylorus Wall structure • Basically the same wall structure as the entire gastrointestinal tract: tunica mucosa, tela submucosa, tunica muscularis, and tela subserosa and tunica serosa. • Exception: tunica muscularis consists of three layers: fibrae obliquae, stratum circulare and stratum longitudinale (important for peristaltic motion). • Tunica mucosa contains specialized glandular cells that produce HCI and intrinsic factor (parietal cells), pepsinogen (chief cells; protein digestion) and mucus (surface epithelial cells and accessory cells, mucin-producing; protection against self-digestion). Neurovascular structures (see also p. 407) Upper abdominal circulation. • Arteries: owing to the location in the upper abdomen, all aa. gastricae arise directly (a. gastrica sinistra) or indirectly (through the a. hepatica communis or a. splenica) from the truncus coeliacus: aa. gastricae sinistra and dextra supply the curvatura minor, aa. gastroomentales sinistra and dextra supply the curvatura major; variably an a. gastrica posterior for the paries posterior of the gaster. • Veins: vv. gastricae sinistra and dextra, vv. gastroomentales sinistra and dextra, v. prepylorica and vv. gastricae breves directly or indirectly (v. splenica or v. mesenterica superior) into the v. portae hepatis • Lymphatic drainage: through groups of nodi lymphoidei at the curvatura minor (nll. gastrici sinistri and dextri), curvatura major (nll. gastroomentales sinistri and dextri), and at the pylorus (nll. pylorici) into the nll. coeliaci and from there into the cisterna chyli • Autonomic innervation: – parasympathetic through the two nn. vagi (trunci vagales) – sympathetic, primarily through the n. splanchnicus major and partially through the nn. splanchnici minores (through the ganglia coeliaca) Function • Temporary reservoir for food, hence its large volume (1.2–1.8 L) and high elasticity. • Start of digestive process requirements: – production of gastric juice containing HCl (approximately 2 L per day, responsible for protein denaturation and sterilizing food, HCl concentration 5 M/L) and protein-digesting enzymes (pepsin) – liquefaction and mechanical grinding (through peristaltic motion of the paries gastricus) of food into chyme which is passed in small amounts through the pylorus to the duodenum. Peristaltic transport of chyme – secretion of intrinsic factor for the intestinal resorption of vitamin B12 Embryonic development • Of endodermal origin, derived from the praeenteron. • The gaster has a mesogastrium dorsale and a mesogastrium ventrale that develop into the omentum majus and minus, respectively. • As the gaster and the mesogastrium rotate, the hepar and splen shift to the right and left upper quadrants and the duodenum comes to lie retroperitoneally. Major diseases • Acute and chronic inflammation (gastritis) • Ulcer (often caused by a type of bacteria called Helicobacter pylori) • Malignant gastric tumor (gastric carcinoma) Location • Largely secondarily retroperitoneal in the right upper quadrant just below the hepar, with approximately 2 cm of the superior part in proximity to the gaster remaining intraperitoneal. • As a result of the tilt and rotation of the gaster during embryonic development the duodenum shifts to the right, superior and posterior. Shape and parts of the duodenum • Hollow, tubular organ, in anterior view: c-shaped • Shortest segment of the intestinum tenue and has a length of approximately 12 finger-widths • 4 parts from top to bottom: – pars superior – pars descendens – pars inferior or horizontalis – pars ascendens Wall structure • Basically the same wall structure as the entire gastrointestinal tract: tunica mucosa, tela submucosa, tunica muscularis (with strata circulare and longitudinale), tela subserosa, and tunica serosa or adventitia, with the plicae longitudinales duodeni being the most distinct and diminishing in size toward the end of the intestinum tenue. • Tunica mucosa with specialized circular folds (also known as Kerckring’s folds). Gll. duodenales (also known as Brunner’s glands) open into the intestinal lumen.

23.2 Pericardium
23.3 Cor (Heart)
23.4 Trachea, Bronchi, and Lungs
23.5 Oesophagus
23.6 Gaster (Stomach)

23.7 Intestinum Tenue: Duodenum
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine
